With the pandemic, Neil Warshawsky, DDS, has taken consults, appointment check-in, and treatment monitoring virtual.
By Alison Werner | Photography by Mark Segal Photography
Pivot or perish: No phrase better describes the last 6 months for small businesses across America. Local coffee shops started doing delivery and stocking pantry items. Bookstores started offering curbside pickup. And hair salons started offering haircuts in the parking lot.
Small businesses everywhere have had to change the way they do business to stay alive, including orthodontic practices like Get It Straight Orthodontics, the Chicago-based practice of Neil Warshawsky, DDS.
When the closure order came in March, Warshawsky knew instinctively that financial survival would require he pivot—a lesson learned weathering both the 2008 recession and 2012 market crash. During both those periods of financial uncertainty, he made a calculated decision to invest heavily in his own practice. He knew he couldn’t control the economy, but he could control the business he’d spent years building.
Once the doors closed, Warshawsky embarked on a project that would completely change how prospective patients first engaged with the practice and how current patients would receive care: He took the practice virtual.
A virtual practice had been on Warshawsky’s to-do list, but prior to COVID-19, it was about 2-years out. Get It Straight Orthodontics had always been tech-heavy—intraoral scanners, cone-beam, digital charts, etc, and Warshawsky knew using virtual technology, including remote monitoring, was the next step. With COVID, the project became priority #1.
Seven months into it, the venture generated record level starts from the internet and translated into efficiencies that help the practice manage reduced scheduling requirements.
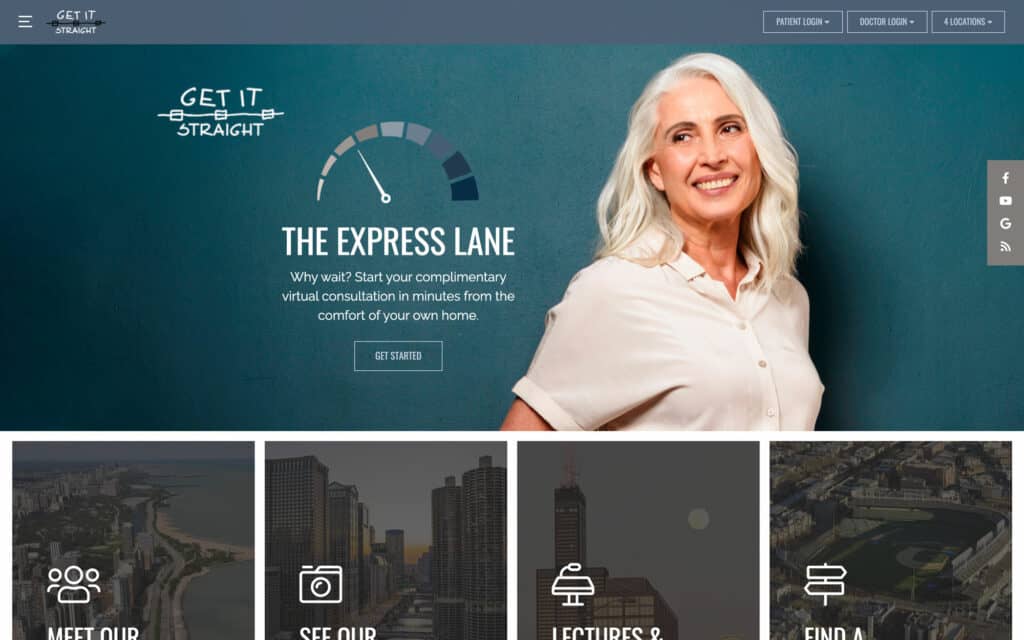
Start with the Website
The virtual practice started with a complete redesign of the practice’s website. The goal with the virtual practice was twofold: connect with potential new patients during closure and beyond and maintain his connection with existing patients. The changes are most noticeable on the website’s mobile and tablet versions. Site visitors immediately get a call to action button on the bottom of the screen, whether they are a patient or not, offering two options: a virtual consult or curbside check-in. As Warshawsky puts it, with the virtual consult, “Anybody surfing me, automatically realizes they can talk to me for free. It’s awesome.”
The rollout of the virtual practice component was coupled with a targeted advertising buy created by an ad agency. Resistant to the idea at first, Warshawsky ultimately realized it was necessary to keep his volume up once he reopened. The Facebook ads draw on that company’s user data to build profiles of the type of patients the practice wants to see and then targets them within a certain radius of one of the office’s four locations. In conjunction with the targeted Facebook ads, Warshawsky started doing a Facebook Live every Monday. Warshawsky is quick to admit he was pretty bad at it, but with that came humor. During one session he was shocked to see 327 people watching. “That’s what taught me social media is a real form of communication. I was just amazed at how many people were starting to rely on it to listen to us,” he shares. The practice started putting out creative content on a weekly basis during closure and continues to this day.
The results of the targeted ads coupled with the virtual visit tool on the practice’s homepage blew Warshawsky away.
“I had no idea how many people would reach out virtually,” he shares. “In our first 14 days after we reopened, we booked and started $35,000 worth of work off the internet.” Warshawsky adds that the majority of those starts came from direct visits to his website rather than Facebook.
The practice dedicated an email account to virtual consults and Warshawsky continues to dialogue daily with people, responding to email whenever he has a free moment. When someone makes the effort to send five photos, Warshawsky downloads them into his treatment planning software and records his screen and an audio message explaining what he sees. More often than not, those patients start.
Of those patients who go the virtual consult route: “Some are just high school kids or young adults with low self-esteem, and some are adults who have been avoiding orthodontics for fear or vanity reasons. Wearing a mask is the perfect impetus to cause someone vain to finally do their orthodontic care. It’s been a lot of fun, but it’s also a lot of work to keep up with everyone’s expectations.”
Managing the Virtual Component
To manage the increased workload, Warshawsky has made additional changes in recent months. He switched to Dolphin Imaging & Management Solutions’ practice management software to track the images submitted as part of the virtual consults. As Warshawsky puts it, the Dolphin software will create a time point when the image is uploaded, giving the practice a more accurate patient history. Another reason for the switch was to give patients the ability to make their own appointments from their mobile device.
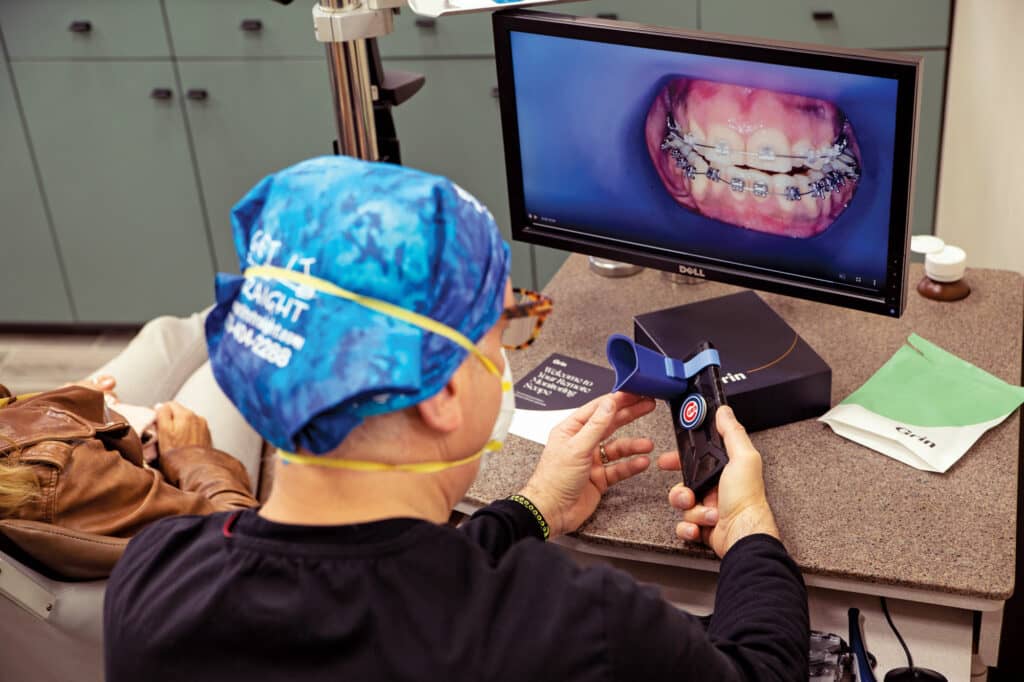
The biggest technology adoption related to the virtual practice and existing patients, however, is the integration of the remote monitoring platform from the teleorthodontic company Grin. Developed by longtime friend and fellow orthodontist Adam Schulhof, DMD, the company’s founder and CEO, the Grin Remote Monitoring Platform consists of the Grin App and the proprietary Grin Scope, an FDA-listed medical device designed to serve as an intraoral adapter. Affixed to the patient’s smartphone, the Grin Scope retracts the cheeks in order to allow a full view of a patient’s mouth. The patient self-scans their teeth using the Grin App which guides them through the experience. Once scanned, orthodontists use the video to assess the patient’s treatment progress via their Grin online doctor portal.
Reducing Exposure Risk
Since reopening, Warshawsky’s goal has been to limit risk of COVID exposure for both his staff and patients. And one way to do that is limit patient appointments whenever possible, while maintaining doctor supervision. The Grin platform allows the patient to send Warshawsky a good quality intraoral video scan—whether they are being treated with braces or aligners. Once the patient sends in the video, the doctor is alerted, and they can then have a conversation via text. One aspect of the app that Warshawsky appreciates is that the patient can pull up their own records on their cellphone and they can talk about treatment progress with the progress images in hand.

Meanwhile, the Grin Scope is able to capture the intraoral area from a number of angles. “The one thing I’ve learned after 22 years of clear aligner therapy is you need to see things from a lot of angles,” Warshawsky says. “Whether you’re designing therapy or you’re monitoring therapy, you need to see it from a lot of different angles, specifically to see if torque is under control.”
Beyond limiting COVID exposure, the practice’s remote monitoring capability gives those patients who don’t want to come to the practice often—the ones who might otherwise go the direct-to-consumer route or the ones who are worried about their COVID exposure like the mother of a young girl who wants to keep her daughter out of the office for as long as possible—an alternative that keeps them under an orthodontist’s direct care.
In the case of the young girl, when the doors opened up on a bracket, Warshawsky was able to spot it and have her come in to stop the tooth falling backwards. The benefit of seeing what was happening in advance of the appointment: Warshawsky could plan ahead and have a setup ready to place three additional brackets at the appointment, eliminating the need for an additional appointment.
Emphasizing that direct care and case control is key with this workflow, says Warshawsky, “it’s important that patients understand how critical it is that I’m watching them. But more important than that control is for the patient to actually believe I’m doing them a service. When the patient really believes that, they’re less apprehensive and the case runs better.”
Warshawsky’s plan is to make the Grin platform part of the practice’s DNA. He’s started by giving the Grin Scope to all new cases, as well as cases that need additional monitoring—and he’s doing so at no additional charge. Warshawsky admits his workflow around the remote monitoring and virtual consults is a work in progress. In a month, his practice typically sees about 1,600 patients. His goal is to shift 30% of those patients to remote monitoring going forward. The plan is to allot time in his schedule throughout the day to the virtual consults and remote monitoring follow-up calls, which average about 5 minutes.

The New Patient Experience
When Warshawsky was working on that website redesign, he had the foresight to add a mobile curbside check-in system that patients could access on the website from their smartphone while parked in their car. The feature utilizes two-way texting, another project Warshawsky moved up during closure.
The transition to two-way texting was easy, says Warshawsky who had questioned the tool’s utility prior to implementation. “Here today, I am confessing that I was wrong. It’s an incredibly useful tool and it’s not costly at all,” he says.
The front office staff uses the two-way texting to communicate with patients throughout the day, but during curbside check-in, the tool allows the office to communicate with the patient/parent outside and to provide them with an online COVID survey. That survey is completed before they come through the front door. It’s then saved by the practice to ensure traceability.
A designated greeter—a new role in the practice—then meets the patient at the door. The greeter takes and records their temperature and pulse oximetry. From there, an assistant picks up the patient and walks them back to the chair.

Customizing Efficiency
Throughout the COVID pandemic, Warshawsky’s treatment philosophy has remained consistent: customization. That means he maintains a full arsenal of treatment modalities to meet the needs of each patient. The practice offers aligners—3M Oral Care’s Clarity Aligners and Invisalign—and 3M self-ligating and lingual braces, as well as a number of surgical options, including Wilckodontics and TADs. The practice also uses soft pulse vibration and micro-osteoperforation (MOP) with Propel. The result is a big practice with a boutique type feel. “We are customizing the physiology to our patient’s needs,” says Warshawsky, who, prior to COVID, could be found lecturing and teaching across the country more than 40 times a year.
To illustrate how he translates his treatment philosophy into action and the boutique feel, Warshawsky shares the story of an IT trainer he was working with as part of his job managing the orthodontic section at the Craniofacial Center at the University of Illinois Health Center. As the two worked, the trainer asked Warshawsky if he would take a look at his teeth. The man pulled down his mask and Warshawsky started taking photos. The trainer had a full unilateral crossbite. When Warshawsky asked where he lived, the trainer said Florida—a no travel state for Chicago currently. But, the trainer added, he travels frequently for work and is on the road months at a time.
“Honestly, it doesn’t matter where you live,” Warshawsky told the trainer. “We can manage your case from anywhere.” He then set to customizing a treatment plan that included a full set of braces, a maxillary skeletal expander, a non-surgical option given the trainer’s time on the road, and a Grin Scope.
“He comes back for another round of training with us in a month, so I’ll see him then. And after that, hopefully, we’ll see him every 3 to 4 months. I don’t expect more than four wires on him—five at most,” says Warshawsky, who completed both dental school and his orthodontic residency at the University of Illinois. “Sometimes [the treatment plan] is about what makes sense. [This patient] is on the road a lot, so I gave him a solution that fit.” The plan is for the patient to shoot an intraoral video with the Grin Scope every 2 weeks to allow Warshawsky to track the expander. And if there is an emergency and the patient is not in the Chicago-area, Warshawsky will refer him to another doctor.
Coming Through Stronger
COVID-19 has placed a new emphasis on finishing orthodontic cases efficiently. Yes, that has always been the goal, but now there is a new impetus according to Warshawsky.
“If you can get your job finished in five less visits, then you’re doing everybody a service, because that’s five times your staff won’t be exposed. That’s five times the patient won’t be exposed.”
Warshawsky admits that before COVID, his practice was often guilty of defaulting to, for example, visits every 6 weeks for self-ligating patients, when every 8 weeks would have been better, especially to let the wire technology fully express. Now with the need to minimize everyone’s COVID exposure risk and the need to have more slots for new starts, Warshawsky is fully trusting both the remote monitoring and the mechanics he’s chosen for his patients.
“I want to be able to come through this whole COVID crisis stronger, with everybody still loving what they do and not fearful of going to work. I want the patients to understand that we’ve created a healthy environment where not only do we take their safety as a paramount precaution here, but we still deliver the best care possible.” OP
Alison Werner is chief editor for Orthodontic Products.