The new Invisalign Palatal Expander innovates maxillary skeletal expansion with a custom, removable, no-screw device that allows for a digital workflow, fewer appointments, and improved oral hygiene during treatment.
By Sandra Khong Tai, BDS, MS, Cert Ortho, FRCD
Maxillary expansion is a common treatment modality where there is maxillary skeletal constriction, with or without the presence of unilateral or bilateral posterior crossbite. In the current orthodontic landscape, orthodontic expanders usually incorporate a screw type device that may be removable, with an acrylic plate, or fixed to bands on the permanent first molars and other posterior teeth. Some expanders may even be supported by temporary anchorage devices. All require turning the screw to activate the expander.
Introduction to the Invisalign Palatal Expander System
In the latest innovation, combining the sophistication of advanced software algorithms, 3D printing and digital technology, Align Technology has launched a 3D printed, nylon palatal expander called the Invisalign Palatal Expander (IPE) System. It consists of a series of 3D-printed expanders, which follow the curvature of the palate and cover the three posterior teeth: first primary molar (or first premolar), second primary molar (or second premolar) and permanent first molars. Each expander has an activation of 0.25 mm, and is designed to be worn full time, even while eating and drinking, and changed daily or every other day according to the orthodontist’s prescription.
The system also includes the Invisalign Palatal Holder, which is designed to hold the maxilla post-active expansion until the patient is ready for the next treatment phase.
There are many distinct advantages to this expander, such as
- It is removable. This enables the patient to brush and floss the teeth under the expander, thus maintaining oral hygiene.
- It follows the curvature of the palate. The custom curvature makes the expander very comfortable and means no dietary restrictions.
- No turning of the screw is required. The expander is activated by simply changing up to the next expander.
Clinical Case Report
Chief concern: Unilateral posterior crossbite and lower arch crowding
A 10-year-old male presented in mixed dentition with a Class I malocclusion. The chief concern was a unilateral posterior crossbite and lower arch crowding. There was an increased overjet of 4 mm and a deep overbite. In the upper arch, permanent lateral incisors were still unerupted. There was lower incisor crowding present. A unilateral posterior crossbite was noted on the right side, with lower midline deviation and a functional shift to the right (Figure 1 and 2).



Figure 1: Pre-treatment intraoral photographs.

Figure 2: Pre-treatment intraoral scans, showing the posterior crossbite on the right buccal.
Treatment objectives
The treatment objectives were maxillary expansion to correct the posterior crossbite and eliminate the functional shift. The upper and lower dental arches would be aligned, with the dental midlines aligned with facial midlines. The upper median diastema would be closed, and space created for the eruption of the maxillary lateral incisors.
Treatment with the Invisalign Palatal Expander
The Invisalign Palatal Expander was used for expansion (Figure 3). Attachments were placed on the maxillary primary second molars and permanent first molars. The patient wore the IPE full time, including eating and drinking, and removed it once a day to brush and floss and then when the next expander was inserted. Each expander had an activation of 0.25 mm. The patient was monitored every 2 weeks. During treatment, the patient maintained outstanding oral hygiene, and no inflammation in the palatal or gingival tissues, demineralization, or caries were observed on the teeth under the expander.

Figure 3: The Invisalign Palatal Expander: intraoral views.
Expansion completed
Expansion was considered completed when the lingual cusps of the maxillary permanent first molars touched the buccal cusps of the mandibular permanent first molars. The posterior crossbite had been corrected and the functional shift eliminated. This was achieved after 32 days (Figure 4 and 5).


Figure 4: Intraoral photographs on completion of expansion at 32 days.

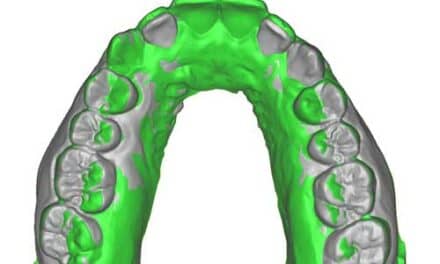
Figure 5: Intraoral scan views post expansion, showing the lingual cusps of the maxillary first molars touching the buccal cusps of the mandibular first molars. Note the change in shape of the palate and the increase in median diastema.
Retention
The patient was then scanned for the Invisalign Palatal Holder, which is essentially a series of passive expanders, designed to maintain the maxillary expansion achieved. The palatal holders were worn full time and changed every 2 weeks for a retention period of 12 weeks. After 8 weeks of retention, the patient returned to the office and was scanned again with the iTero Element 5D Plus scanner, for continuation of treatment with Invisalign First aligners. The holder was then re-inserted and full time retention continued for another 4 weeks.
Invisalign First
Invisalign First aligners were inserted at the 12-week mark to close the upper median diastema and create space for eruption of the maxillary lateral incisors. Buccal root torque of the maxillary molars was added. The upper arch form was developed to create an ovoid arch form. The lower arch was also expanded with Invisalign First to coordinate with the newly expanded upper arch and the lower incisors aligned. After the first series of 26 aligners were worn, the maxillary lateral incisors had erupted. Fifteen additional aligners were made to align the lateral incisors and complete treatment. The patient was then placed into nighttime retention with retainers. Total treatment time was 14 months with 32 days of expansion, 12 weeks of full-time retention, and 26+15 Invisalign First aligners.
Final occlusion
In the final occlusion, both upper and lower dental arches were aligned. The posterior crossbite and functional shift had been eliminated. Both upper and lower dental midlines were coincident with the facial midlines (Figure 6).
Intraoral scans of the palate, pre-treatment, after active expansion, and after treatment with Invisalign First are shown for reference in Figure 7.


Figure 6: Post-treatment intraoral photographs.



Figure 7: Intraoral scans pre-treatment, after active expansion, and after treatment with Invisalign First.
Case discussion
Treating this young patient with the Invisalign Palatal Expander system was a seamless experience. The IPE system achieved the required amount of expansion planned. Skeletal expansion was achieved with the separation of the maxillary incisors and an increase in the space between the two central incisors.
This treatment did not generate any complications or emergency visits. The patient did not present any speech issues, dietary restrictions, or food impaction under the expander. The patient was compliant and removed the appliance for flossing, brushing, and washing the device only. Parents did not have to activate the device; the child simply placed a new expander every night.
Invisalign Palatal Expander Changes Case Approach
The IPE changed how we approach cases requiring palatal expansion. During consultations, we show patients and parents a conventional Hyrax expander and an Invisalign Palatal Expander system sample. Each time they chose the IPE without hesitation.
From the clinician perspective, advantages of the IPE include a simplified digital workflow with fewer appointments. An intraoral scan is captured and a prescription for the IPE is submitted. This eliminates the multiple appointments required in conventional expanders where separators have to be placed and molar bands fitted, followed by the insertion appointment. This latest innovation from Align Technology heralds a new digital era for maxillary skeletal expansion. OP

Sandra Khong Tai, BDS, MS, Cert Ortho, FRCD, received her specialty training in orthodontics at the University of Minnesota. She is a clinical assistant professor at the University of British Columbia and adjunct clinical assistant professor at the University of the Pacific. She is the author of the textbook Clear Aligner Technique (Quintessence Publishing 2018) and has treated over 4,500 cases with clear aligners. She is a diplomat of the American Board of Orthodontics.