

ABCs of a Better Ceph
Steven Astuto, DDS
Amarillo, Tex

- A line of demarcation is caused by the patient taking a breath.

- The patient is looking up, creating an incorrect angulation.
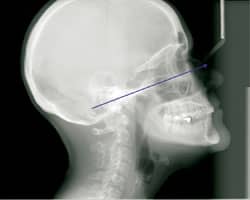
- In the ideal ceph, the patient looks straight ahead and holds his breath.

Thanks to this new age of digital imagery, processing errors are a thing of the past for most of us. Gone are the days of green films with roller marks that remind us to change the solutions in the processor or the occasional film with a big black abyss that appears if the film was accidentally previously exposed. Thank goodness for technology and the efficiency it affords busy orthodontic practices. Now, instantaneous images offer quick diagnoses with increased accuracy.
Of course, with new technology comes new challenges in the way that these images need to be captured in order to get the maximum benefit of digital imagery. One such example is in the area of taking lateral cephalometric views. With our old, film-based ceph machine, the image was taken in a very short period of time, usually less than a second, because the x-ray field was greater. However, new ceph machines expose less radiation because of greater collimation and smaller x-ray fields. The Planmeca Promax takes cephs using two linear beams that travel laterally from nose to spine, converging along Frankford Horizontal. The time to take this view ranges from 18 seconds for very fine views to 9 seconds for fine views.
In the first ceph displayed, the angle is pretty good. The occlusion and Frankford Horizontal are parallel to the floor. The KVP and MA settings are sufficient. However, you can see a definite line of demarcation along Frankford Horizontal. The patient had taken a deep breath as the beam passed, not allowing the beams to converge seamlessly.
This can be corrected by ensuring that the patient remains as still as possible while the radiograph is being taken.
To make your digital cephs the best diagnostic quality possible, remember the ABCs of a better ceph:
- Angle: Make sure your patient’s occlusion is parallel to the floor. Avoid stretching your patients upward or having them stand with their chin tucked. Both of these things can affect angulation.
- Breath: Hold it! Asking patients to hold their breath during the exposure eliminates a lot of movement.
- Correct Settings: Check your KVP and MA settings. Are they sufficient for the college linebacker or too strong for the small 8-year-old?
Remembering your ABCs will help you get the most out of your digital cephs.

Aligners Versus Retainers

- Do you have a pearl to share with your colleagues? Please send it to along with your headshot and any other pictures you would like to include.

Roy King, DDS
Jupiter, Fla
As we all know, if a retainer is not worn for 1 week, it may no longer fit the patient properly when he or she tries to use it again. If you can identify the patient ahead of time before removing the braces, I would recommend making that patient a maxillary Inman Aligner instead of the conventional maxillary removable retainer. The beauty of this is that if you get any type of rotations or movement of the maxillary anterior teeth, the Inman Aligner will always fit properly and will move those teeth back into their proper position. Because it uses a Nitinol coil spring, the force is so gentle that it will not displace the retainer from the maxillary arch, which has been a recurring problem when using springs made of stainless steel wire.








