By offering a noninvasive accelerated orthodontic treatment solution to patients requesting faster and more comfortable treatment, orthodontists are simultaneously improving patient satisfaction and increasing practice efficiency without compromising the quality of their clinical results. However, from lecturing around the country and reading the literature, I’ve learned that too often orthodontists are unable to realize these benefits because they’ve coupled innovative technology with outdated treatment protocols. Specifically, orthodontists using traditional fixed bracket cases have failed to alter their wire sequencing and appointment intervals in order to effectively and efficiently realize the benefits of accelerated orthodontic treatment. The cases in this article demonstrate an example of how to adjust wire sequencing protocols when using a self-ligating bracket system and low pulsatile forces to enhance the rate of tooth movement.
In my private practice, I use the Forestadent FACE Evolution self-ligating bracket system (Forestadent) and AcceleDent® (OrthoAccel Technologies Inc) as my standard treatment appliances. An FDA-cleared noninvasive vibratory orthodontic device, AcceleDent increases osteoblastic activity while reducing hyalinization formation to allow for quicker tooth movement during the early stages of treatment. Randomized clinical trials have shown that AcceleDent speeds up tooth movement by as much as 50% during orthodontic treatment and reduces discomfort by up to 71%.1-2 While clinical evidence for self-ligating brackets hasn’t shown a statistically significant difference in treatment time when compared to traditional twin brackets, the mean average shows that self-ligating brackets speed up treatment by 2 months.3 But statistical significance alone cannot convey the complete picture of the effectiveness of an intervention. Two months is a significant gain from the patient perspective—compare the emotional response when telling patients they have completed treatment 2 months faster to telling them they have to wear their braces for 2 more months. Additionally, evaluating the effectiveness of self-ligating brackets and AcceleDent is inconclusive if orthodontists are not modifying their wire sequencing protocols to account for accelerated tooth movements.
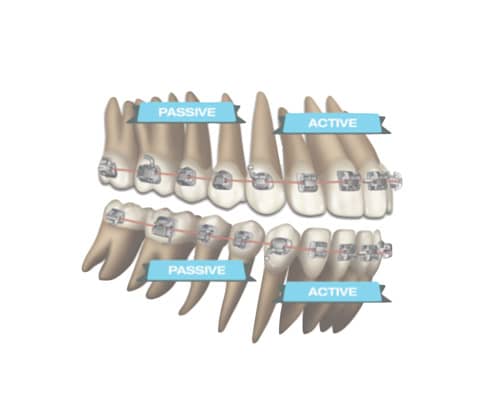
Figure 1
The Mechanics and Treatment Approach
With the Forestadent FACE Evolution system, I’ve adopted a unique hybrid approach of using active and passive appliances simultaneously. The active appliances are placed cuspid-to-cuspid and the passive appliances are placed on the posterior segments (Figure 1). By placing active appliances in the anterior region, I gain three-dimensional control of the inclination of upper and lower incisors as I progress through my archwires. With an .022 slot case, I can place an .020 square wire to provide inclination control earlier in treatment. In the posterior, the passive self-ligating appliance allows more efficiency with sliding mechanics and less binding in the posterior segments.

Figure 2
Patients are instructed to use their AcceleDent for 20 minutes daily throughout treatment (Figure 2). By gently biting on the device’s acrylic mouthpiece while the device is active, AcceleDent’s low pulsatile forces engorge the blood supply in the craniofacial sutures and stimulate bone movement at the cellular level.4
Together, the low pulsatile forces and the self-ligating brackets significantly accelerate tooth movement during the leveling and aligning phase (Stage 1). I recommend beginning with the largest NiTi wire possible (.014 or .018 NiTi) and advancing to the .020 x .020 NiTi. Brackets are reset as needed and second molar bands or tubes are placed. The variability is the amount of crowding. The Stage 1 goal is to progress to the .019 x .025 stainless steel wire in less than 4 months. In order to achieve this, wire change appointments should occur every 4 weeks. Teeth are moving very fast during Stage 1 so it’s important to take advantage of the movement and mobility of teeth. Do not let patient appointment intervals extend beyond 6 to 8 weeks as is protocol with standard treatment. This is why statistical studies may show little difference in comparing the rate of tooth movements in 6-to-8-week intervals. If the mechanics are not altered to accommodate faster tooth movements during Stage 1, the clinical efficiencies will be negligible. When a wire has done its work, it becomes passive, and as a result, teeth and tooth movements wait until the next force delivery system is applied.
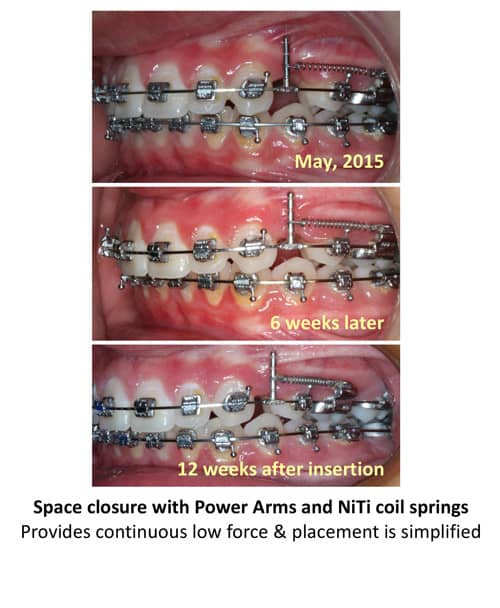
Figure 3
During Stage 2, the working phase, teeth move more rapidly than usually expected. The .019 x.025 stainless steel wire (the working wire) is used to address the anterior-posterior, transverse, and vertical movements. Patients during this phase are seen every 6 to 7 weeks. For space closure, I currently use NiTi springs exclusively. Several images in these cases show a double key hole loop; however, with our current mechanics we use NiTi springs (Figure 3). Space closure with maximum anchorage may take 8 to 10 months and with reciprocal anchorage may take 4 to 8 months. The variabilities in Stage 2 include the patient’s overbite and overjet, transverse tooth positions, vertical controls and patient cooperation with elastics or headgear.
Stage 3, the finishing stage, begins when molars are Class I, the overjet/overbite is within 2 mm of optimal occlusion, and there are no intra-arch spaces or lateral open bites greater than 2 mm. The goal is to achieve a mutually protected occlusion and a balanced profile with smile aesthetics. One of the primary benefits of adjusting the wire sequencing in Stages 1 and 2 is that orthodontists arrive at Stage 3 faster, allowing sufficient time for finishing and detailing. Stage 3 mechanics include resetting brackets as needed and placing the largest NiTi wire possible where the self-ligating bracket clips can close and progress to the .0195 x .025 stainless steel wire. Finish with multistranded wires. The goal is to complete Stage 3 in less
than 4 months.
When examining these cases, note the difference in treatment protocols and compare them to twin bracket, non-accelerated cases to estimate how much treatment time is being saved and how much clinical efficiency is being achieved.
Case Study: Patient 1
[metaslider id=31075]
An 11-year-old female diagnosed with Class I/II, crowding, narrow arches, deep bite, partially erupted tooth.
Projected treatment time: 24 months.
Mechanics used: Self-ligating active anterior bracket and passive posterior bracket; extraction of four bicuspid teeth; headgear (PM); AcceleDent.
Treatment approach and wire sequencing was as follows:
Stage 1 (level/align; 3.25 months): Day 1: .014 NiTi > .020 square NiTi. 2.5 weeks: U: .020 square NiTi, L: .018 NiTi. 7 weeks: .0195 x .025 NiTi. Reset brackets as needed and band 7s. .0195 x .025 NiTi. Appointment/wire changing intervals: every 4 weeks.
Stage 2 (working; <11 months): .0195 x .025 SS. Note: Prior to adopting the NiTi springs protocol, double key hole loop was used. Class II elastics on right side. Appointment/wire changing intervals: every 6 to 7 weeks.
Stage 3 (finishing; 3.5 months): Reset brackets as needed. .0195 x .025 NiTi > .0195 x .025 SS. Nighttime triangular elastics. .0195 x .025 multistranded wires
Total treatment time: 17.75 months. Some scheduling limitations due to parent’s schedule. No radiographic sign of root resorption. Note: The extractions did not result in retraction. The vertical held with nighttime headgear, self-ligating brackets, and AcceleDent. These mechanics kept the upper molars up and prevented the lower molars from extruding. The stainless steel wire allows the orthodontist to dictate the arch form.
Case Study: Patient 2
[metaslider id=31102]
A 14-year-old female patient diagnosed with Class I, crowding, impacted UL3, anterior crossbite, mild facial protrusion.
Projected treatment time: 22 to 24 months.
Mechanics used: Self-ligating active and passive hybrid bracket system; extraction; and AcceleDent.
Treatment approach and wire sequencing was as follows:
Stage 1 (level/align; 3+ months): .014 NiTi > .020 square NiTi. 4 weeks: U: .020 square NiTi, L: .018 square NiTi; reset brackets as needed and band 7s. Extracted the impacted upper cuspid and 3 remaining bicuspids. 8 weeks: .0195 x .025 NiTi. Appointment/wire changing intervals: every 4 weeks.
Stage 2 (working; 8 months): U: .0195 x .025 DKH, L: .0195 x .025 SS. Posted hooks with NiTi springs. Triangular elastics as needed. Appointment/wire changing intervals: every 6 to 7 weeks.
Stage 3 (4 months): Reset brackets as needed. .0195 x .025 NiTi > .0195 x .025 SS. Triangular elastics. .0195 x .025 multistranded wires.
Total treatment time: 15 months. No radiographic sign of root resorption.
Case Study: Patient 3
[metaslider id=31103]
An adult female diagnosed with Class I, crossbite at the lateral incisor area, edge-to-edge bite, and previously extracted upper left bicuspid. Mounted casts show she has a mild discrepancy between her intercuspation and seated condylar position with approximately 10% facet wear of the incisors due to her edge-to-edge bite. A diagnostic wax setup was done to determine the maximum amount of space that could be gained during orthodontic treatment for prosthetics.
Projected treatment time: 16 to 18 months.
Mechanics: Self-ligating active appliance cuspid to cuspid and passive appliance in the posterior segments; re-establish space in upper left bicuspid area for replacement tooth; and AcceleDent.
Treatment Approach & Wire Sequencing
Stage 1 (level/aligning; 3 months): .014 Copper NiTi > .020 square NiTi; light Class III elastics worn at night; reset brackets as needed and banded 7s; .0195 x .025 NiTi. Appointment/wire changing intervals: every 4 weeks.
Stage 2 (working; 4 months): .0195 x .025 SS. Appointment/wire changing intervals = every 6 to 7 weeks.
Stage 3 (finishing; 5 months): Light vertical elastics and some step-down bends in a flexible wire; reset brackets as needed; .0195 x .025 NiTi > .0195 x .025 SS; .0195 x .025 multistranded wires
Total treatment time: 12 months, 2 weeks. No radiographic sign of root resorption. Patient chose to wear clip on prosthetic until restoration decision is made. OP
References
- Pavlin D, et al. Cyclic loading (vibration) accelerates tooth movement in orthodontic patients: A double-blind, randomized controlled trial. Seminars in Orthodontics. 2015; 21(3): 187-194.
- Lobre W, et al. Pain control in orthodontics using a micropulse vibration device: A randomized clinical trial. The Angle Orthodontist. 2016; 86(4): 625-630.
- Machibya FM, et al. Treatment time, outcome and anchorage loss comparisons of self-ligating and conventional brackets. The Angle Orthodontist. 2013; 83(2): 280-285.
- Vij K, Mao JJ. Geometry and cell density of rat craniofacial sutures during early postnatal development and upon in-vivo cyclic loading. Bone. 2006; 38(5): 727-730.
 Straty Righellis, DDS, graduated from UCLA Dental School and received his orthodontic specialty certification from the University of California, San Francisco. He maintains a private practice in Oakland, Calif, and serves as an associate clinical professor at the University of the Pacific and the University of California, San Francisco. Righellis is a diplomate of the American Board of Orthodontics, is on the editorial review board for the American Journal of Orthodontics, and lectures around the world on excellence in clinical orthodontics.
Straty Righellis, DDS, graduated from UCLA Dental School and received his orthodontic specialty certification from the University of California, San Francisco. He maintains a private practice in Oakland, Calif, and serves as an associate clinical professor at the University of the Pacific and the University of California, San Francisco. Righellis is a diplomate of the American Board of Orthodontics, is on the editorial review board for the American Journal of Orthodontics, and lectures around the world on excellence in clinical orthodontics.







