
by David R. Musich, DDS, MS, and Matthew J. Busch, DDS
Clinical and communication techniques to help guide long-term treatment


David R. Musich, DDS, MS, and Matthew J. Busch, DDS
The effective treatment of patients with Angle’s Class III malocclusion continues to be a clinical challenge for the orthodontist. Since the Class III growth pattern is frequently part of a familial trait, the orthodontist has a difficult time determining when growth modification is adequate to avoid surgical intervention (Figure 1). It is, however, the orthodontist who must determine if growth modification, dental compensation, and elimination of mandibular functional shifts will be adequate to ultimately avoid a surgical procedure. A number of variables that enter into the final decision and make the orthodontist’s decision extremely difficult are the following:
- Is there additional growth that will undermine the current outcome?
- Is the patient complying with the mechanotherapy to achieve desired growth modification?
- Is additional dental compensation possible to achieve proper incisal relation, and will the patient and the parents accept the facial aesthetic outcome if further dental compensation is needed?
- What are the limits of dental compensation when the Class III skeletal relationship keeps worsening with growth—both functionally and esthetically, both short-term and long-term?
Stellzig-Eishenhauer et al1 made efforts to determine the best cephalometric assessment measurements to differentiate adult surgical Class III patients from adult nonsurgical patients. By narrowing the group studied to adults only, they eliminated the variable of growth and could apply statistical methods to create a predictability equation to assist adult Class III treatment-planning. They assessed antero-posterior deviations and did not include the variables of skeletal transverse maxillary deficiency, crowding, or patient perception of the final facial proportions.
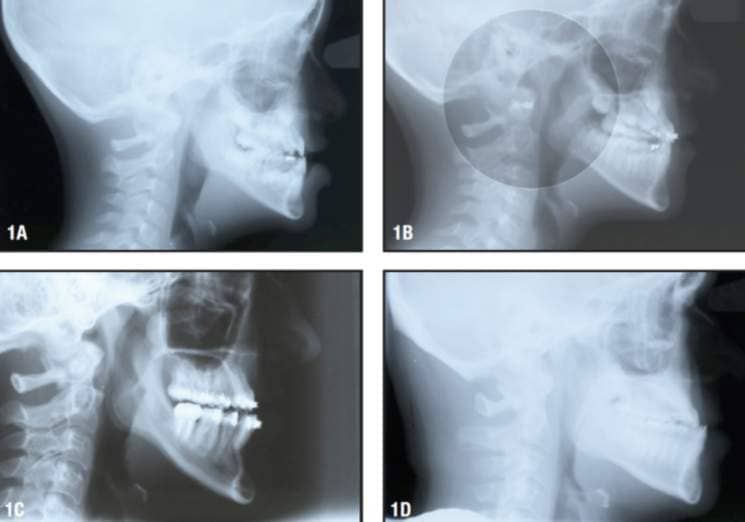
Figure 1: A) Cephalogram of a patient at age 8.5 with a WITS of -9 mm. B) Cephalogram of the patient at age 9.5 after Phase I with RPE and Class III traction—WITS reduced to -6 mm. C) Cephalogram of the patient at age 15.5; unfavorable WITS change (-6 to -12 mm) during pubertal growth spurt delayed Phase II treatment until growth was complete in order to combine orthodontic treatment with jaw surgery. D) Cephalogram of the patient’s father illustrating a clear genetic component to strong skeletal Class III growth pattern—his WITS measures -13.5 mm.
Differential Diagnosis of the Class III Skeletal Problem

Figure 2: A lateral cephalogram of an 8-yearold Class III patient with a radiograph taken in centric relation shows an edge-to-edge bite and an inability to close completely. The incisal interference alters the correct vertical mandibular position, making some cephalometric measurements inaccurate. These inaccuracies make future comparisons less informative. The authors’ recommendation is to take all Class III records in centric occlusion and to include correction of functional shifts, if present, as part of the orthopedic management of the Class III problem.
Guyer and others2 assessed the antero-posterior skeletal components of 144 adolescents using cephalograms, and determined that the Class III malocclusion was caused by several types of maxillary and mandibular imbalances. In addition, several authors have suggested a variety of cephalometric approaches to allow a differential diagnosis.3-6 One of the great difficulties in making a correct diagnosis is that a high percentage of Class III malocclusions have mandibular functional shifts (both forward and sometimes lateral). Many Class III diagnostic guidelines suggest that the initial cephalogram should be taken in centric relation to eliminate the jaw-shift component from the measurements. However, frequently the initial centric relation then has undesirable, error-producing vertical excess due to mandibular closure interference (Figure 2).
Many Class III patients present with an antero-posterior functional shift of the mandible that accentuates the degree of the Class III problem. Therefore, it follows that the elimination of the functional shift is a key part of the “orthopedic” management of the Class III problem. The sooner the forward repositioning of the mandible is corrected, the better will be the growth environment of both the maxilla and the mandible. One of the great benefits of achieving a “seated condylar” position as early as possible for the Class III mandible is eliminating negative forces (“the headgear effect” on maxillary growth) which, if present, make Class III correction more difficult (Figure 3).
Therapeutic Approaches for the Growing Class III Patient

Figure 3: A) Class III malocclusion of 5.5-year-old female illustrating the adverse impact on maxillary growth (“headgear effect”) of occlusal forces each time the lower jaw closes into function. These forces limit maxillary growth in both antero-posterior and transverse planes when there is both an anterior and posterior crossbite. B) Front view of the post-treatment occlusion following early intervention with RPE and Class III traction for 16 months. The goal of Phase I was to eliminate crossbites, to correct anterior alignment, and to replace the adverse “headgear effect” of Class III occlusal pattern with Class I functional forces and achieve stabilization over 4 years. Phase II completion included full braces and more Class III traction from 13.5 to 15.5 years of age.
Based on the findings of Guyer et al, the Class III problem has several anatomic components that participate in the clinical imbalance. It is not surprising that a variety of appliances have been developed by orthodontists to correct the Class III malocclusion. For a period of time, the emphasis of Class III therapy was on stopping the mandible’s growth using a chin cup. About the time orthodontists found that the chin cup had a limited impact,7,8 they became more aware of the maxillary component of the Class III problem and placed more emphasis on modifying maxillary growth.9,10 More recently, the research on Class III correction has focused on the timing of treatment and the use of the reverse-pull face mask.11-13
In the authors’ experience, early Class III management in the primary and/or mixed dentition has more predictable outcomes if:

Figure 4: A) A photographic illustration of the orthodontic removable traction Appliance (ORTA) on a Class III model. This appliance is useful for high compliance (24/7) Class III traction and disarticulation. B) A photograph of the ORTA off the model shows the attached traction hooks in position for Class III traction with the mandible as anchorage. The design of the appliance allows it to be used with reverse-pull headgear when appropriate.
- Compliance is increased by using Class III traction mechanisms that are “user friendly (intraoral),” and can be used in the mixed dentition and/or primary dentition. In the 1980s, Musich developed the orthodontic removable traction appliance (ORTA) (Figure 4). This appliance is used full-time with Class III elastics (6- to 8-ounce) traction, and can be also used in conjunction with a reverse-pull headgear when necessary. In addition to applying Class III traction, the ORTA aids the rapid elimination of the mandibular functional shift, if present, through a disarticulating action that helps to resolve the neuromuscular programming (Figure 5).
- Sutural activation is achieved with a rapid maxillary expander (RPE). Since many Class III patients have had their maxillas restrained by the negative (reverse) occlusal load—sometimes for several years—every effort should be made to accelerate the forward growth of the maxilla. Class III traction 24 hours per day, 7 days per week (using the ORTA and reverse-pull headgear) during the period of expander activation, allows rapid reversal of the maxillary deficiency.
- Interincisal correction—upper incisor reangulation with lower incisor compensation—allows the closure arc of the mandible to be achieved without incisal interference and mandibular forward positioning.
- Assessment of growth vectors at predetermined intervals determine if the original Class III pattern has been overcome with early treatment modalities, and the growth pattern continues in more of a Class I orientation.

Figure 5: A) Pretreatment frontal view of a 6-year-old with significant Class III skeletal malocclusion. B) A frontal view of initial correction showing occlusal coverage expander and ORTA appliance during Phase I therapeutic diagnosis treatment. C) After Phase I, stabilization appliances are in place, and the orthodontist is monitoring Class III growth vectors and dental development. D) The pretreatment cephalogram shows a significant skeletal imbalance of the maxillo-mandibular relationship. E) The patient with reverse-pull headgear in place. The ORTA was worn full-time, and the headgear was worn at night for 9 months. F) A cephalogram taken after Phase I illustrates favorable antero-posterior changes in the maxillomandibular relationship. G) A pretreatment occlusal view of the maxillary arch. H) This expansion appliance cemented to the deciduous teeth present allows for early intervention. I) An occlusal view following Phase I shows improved archform and a lingual arch bonded to four incisors to maintain their stability during ongoing dental development.
Assessment of Treatment Response
It is almost impossible to create a treatment plan for a growing Class III patient and be certain that the outcome will satisfy the functional, aesthetic, and stability requirements that are desirable in orthodontic treatment. Assessing orthopedic response requires accurate initial records, including the following:
- Lateral cephalogram in centric occlusion (this allows the orthodontist to measure the initial position of “B” point, including the amount of antero-posterior functional shift, if present);
- Frontal cephalogram to assess the degree of transverse deficiency of the maxilla;
- Lateral cephalogram of genetically similar parent or grandparent to determine the degree of the familial nature of the Class III problem;
- Wrist film to assess skeletal age and to estimate the number of years of future facial growth; and
- Conventional study records, including study models, photographs, and a panoramic radiograph.

Figure 6: Superimposition (on SN) of 6- and 16-year-old Bolton templates showing the Class I growth pattern of the maxilla and Class I growth of the mandible using growth vector analysis. Red circle “A” shows the growth vectors of maxilla, A point at age 6 to A point at age 16. Red circle “B” shows the growth vectors of mandible, B point at age 6 to B point at age 16.
Class III patients frequently are initially diagnosed by the general or pediatric dentist. Their referral often includes the encouragement that “early intervention may avoid surgical treatment.” Since the long-term treatment response of the growing Class III patient is uncertain, it is then imperative that the orthodontist is able to educate the parents and patient when treatment response is favorable or unfavorable. Without this periodic communication from the orthodontist (or treatment coordinator), the initial uncertainty of the treatment outcome and protracted treatment time may lead to frustration and, as has been reported, subsequent legal action.14
Treatment-response assessment is important in all forms of medical and dental treatment. This is particularly true when a strong genetic component is part of the original diagnosis, and when compliance is an important factor in the outcome. This point was reinforced by Ackerman and Proffit: “We believe that attempts to eliminate uncertainty from orthodontics are laudatory, but at present pragmatism still has an important role in orthodontic practice. Until more reliable diagnostic methods are available, perhaps orthodontists should view the testing of treatment response as a tool rather than a shortcoming.”15

Click to see ORTA guide
– you will need Adobe Acrobat reader to view this.
![]() If you do not have Adobe Acrobat on your computer, you can download it for free from Adobe.com.
If you do not have Adobe Acrobat on your computer, you can download it for free from Adobe.com.
A study of 100 consecutively referred “early treatment patients” found that 15% of patients had a Class III problem.16 Therefore, several of the previously discussed concepts must be integrated when attempting to manage a large number of growing Class III patients. The authors currently use the following integrated approach:
- Take quality initial records, as described above.
- Outline a multiphase treatment plan to the parents/patients.
- Emphasize the treatment-compliance requirements.
- Clarify the re-evaluation mechanism and interval.
- Apply the most reliable Phase I mechanotherapy as soon as possible.
- Incorporate the ORTA for increased hours of Class III traction.
- Incorporate the ORTA for disarticulation, if no other disarticulation mechanism is present.
- Use an RPE for sutural activation of the maxilla.
- Realign and reangulate incisors to correct anterior crossbite.
- Assess treatment response by using the WITS1 measure (the difference between the perpendicular of A point to the occlusal plane and the perpendicular of B point to the occlusal plane) as a reliable guide.
- WITS changes will serve as a horizontally corrected growth treatment response vector (GTRV) (Figure 6).
- Pretreatment WITS compared to the re-evaluation WITS (3 to 4 years after initiation of treatment) will give an indication of the stability of the initial correction.
- Incorporate treatment-response findings into recommendations of further treatment—nonsurgical or surgical, depending on the severity of the WITS differential (Figure 7).
- Create a patient/parent educational mechanism to reinforce the fact that, though orthodontists make every effort to avoid surgery when possible, however, 20% to 40% of patients with Class III malocclusions, when treated as children, are unable to be treated optimally without surgical intervention.
- Periodic communication regarding progress is critical in all Class III treatment situations.
- Sequential, preprinted reports are useful to provide updates to improve patient/parent understanding.
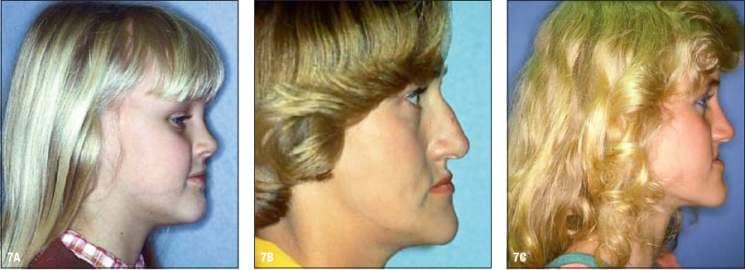
Figure 7: A) A facial profile of a patient who is 6 years, 11 months old and seeking correction of a developing Class III problem. B) A facial profile of the patient’s mother shows mature development of Class III skeletal growth problem. Jaw surgery and orthodontics were needed to correct her Class III problem. C) A facial profile of the patient at 15 years, 11 months shows facial growth changes and development of the mandibular excess problem. D) A cephalometric superimposition of the patient from ages 6 years, 11 months to 15 years, 11 months shows minimal horizontal growth of maxilla and significant horizontal growth of the mandible. E) Cephalometric superimposition of prognathic growth pattern from Bjork and Skieller’s implant studies. The maxillary and mandibular growth vectors are very similar to those of the patient pictured above.


L-Figure 7D, R-Figure 7E
The Limits of Nonsurgical Management
Defining the limits of nonsurgical management is an important issue for both the orthodontist and the parent/patient. How do you avoid overtreatment or undertreatment when prescribing care for the Class III patient who may have several years of facial growth remaining? Since many Class III patients have several diagnostic components contributing to the Class III problem, an effort needs to be made to eliminate both the maxillary deficiency and contributory mandibular functional shifts as early in treatment as possible.
After these corrections have been made, facial growth should be monitored with awareness of the pretreatment WITS measurement, the progress WITS measurement, and the pre-Phase II WITS assessment. By using the WITS measure and its changes as a guide, the orthodontist is making a determination of the GTRV.
Comparing the WITS measurements from McNamara’s study of normal, untreated adult patients and with Stellzig-Eisenhauer’s surgical versus nonsurgical WITS measurements, there is clear indication that a -8 mm to -9 mm WITS differential is reaching the threshold point. When the WITS measurements have negative numbers less than -8 mm, there is high likelihood that a nonsurgical treatment plan can be used to achieve a successful occlusal outcome. When patients with WITS measurements of more than -9 mm are treated nonsurgically, they generally require overcompensation of the incisors, creating unstable incisors positions, facial imbalances, and a compromised occlusal scheme.
Conclusion
Due to the many variables associated with the growing, Class III patient, it is important for the orthodontist to understand as many of the intrinsic and extrinsic variables as possible, and to periodically apply assessment standards to maximize successful outcomes by avoiding overtreatment or undertreatment (Figure 8).
This article represents a synopsis of the assessment of more than 200 “before” and “after” records of treated Class III patients. The authors have noted that there are several keys to success in managing the growing, Class III patient:
- Accept the fact that not all Class III patients can be treated nonsurgically, nor should all Class III patients be automatically considered in the “surgical only” category.
- Use appliances that provide the best orthopedic effect and have the highest potential for compliance.
- Apply a standardized assessment protocol as treatment progresses; the WITS appraisal appears to be a very useful tool to guide the orthodontist and the parent in assessing favorable or unfavorable change in the growth vectors.
- Finally, it is important to provide a mechanism of standardized communication to keep all parties informed as treatment progresses over the 6- to 10-year period of multiphase Class III treatment.

Figure 8: A-C) Right, center, and left bite relationship of a Class III patient prior to any treatment (age 5 years, 6 months). D-F) Right, center, and left bite relationship of the patient prior to Phase II (age 12 years, 2 months). G-I) Right, center, and left bite relationship of Class III patient after treatment completion (age 15 years, 9 months).
David R. Musich, DDS, MS, is in private practice in Schaumburg, Ill. He teaches part-time at the University of Pennsylvania and the University of Illinois, Chicago. He lectures extensively on methods of simplifying the management of complicated orthodontic problems. He is Board Certified, is a past president of the Edward H. Angle Society of Orthodontics, and was the recipient of the AAO’s 2009 Distinguished Service Award.
Matthew J. Busch, DDS, is a Diplomate of the ABO and a lecturer at the University of Pennsylvania School of Dental Medicine’s Department of Orthodontics.
References
- Stellzig-Eisenhauer A, Lux CJ, Schuster G. Treatment decision in adult patients with Class III malocclusion: Orthodontic therapy or orthognathic surgery? Am J Orthod Dentofacial Orthop. 2002;122:27-38.
- Guyer EC, Ellis EE, McNamara JA, Behrents RG. Components of Class III malocclusion in juveniles and adolescents. Angle Orthod. 1986;56(1):7-30.
- McNamara JA. A method of cephalometric evaluation. Am J Orthod. 1984; 86(6):449-469.
- Jacobson A. The proportionate template as a diagnostic aid. Am J Orthod. 1979;75(2):156-172.
- Steiner CC. Cephalometrics for you and me. Am J Orthod. 1953;39:729.
- Pershing M, Katz S, Musich D. Threshold Limits of Non-surgical treatment for the Class III Skeletal Patient. Thesis, U Pennsylvania School of Dental Medicine, Department of Orthodontics, 2005.
- Sugawara J, Asano T, Endo N, Mitani H. Long-term effects of chin cup therapy on skeletal profile in mandibular prognathism. Am J Orthod Dentofacial Orthop. 1990;98:127-133.
- Wendell PD, Nanda R, Sakamoto T, Nakamura S. The effects of chin cup therapy on the mandible: a longitudinal study. Am J Orthod. 1985;87(4):265-274.
- Westwood PV, McNamara JA, Baccetti T, Franchi L, Sarver DM. Long-term effects of Class III treatment with rapid maxillary expansion and facemask therapy followed by fixed appliances. Am J Orthod Dentofacial Orthop. 2003;123:306-320.
- Hagg U, Tse Agnes, Bendeus M, Rabie ABM. Long-term follow-up of early treatment with reverse headgear. Eur J Orthod. 2003;25:95-102.
- Merwin D, Ngan P, Hagg U, Yiu C, Wei SH. Timing for effective application of anteriorly directed orthopedic force to the Maxilla. Am J Orthod Dentofacial Orthop. 1997; 112(3): 292-299.
- Kapust AJ, Sinclair PM, Turley PK. Cephalometric effects of face mask/expansion therapy in Class III children: a comparison of three age groups. Am J Orthod Dentofacial Orthop. 1998; 113(2):204-212.
- Yuksel S, Ucem TT, Keykubat A. Early and late facemask therapy. Eur J Orthod. 2001;23(5):559-568.
- American Association of Orthodontists Insurance Council: Jury awards six-figure verdict to young patient who underwent 8 years of orthodontic treatment.American Association of Orthodontists Bulletin, April, 2004.
- Ackerman JL, Proffitt WR. Treatment response as an aid in diagnosis and treatment planning. Am J Orthod. 1970;490-496.
- Musich DR, Busch MJ. Early orthodontic treatment: current clinical perspectives. The Alpha Omegan. September, 2006.








