By Mart McClellan, DDS, MS
By Mart McClellan, DDS, MS
Whether through photo and video contests, incentive programs, or creative giveaways, during my years in orthodontic practice, I’ve always used innovative methods to keep young patients engaged during the treatment process. In addition, I have recognized the importance of conveying to the parents of these young patients that advancements in technology have greatly enhanced the treatment experience, so that they don’t forgo treatment until it’s too late.
As we are aware (and according to the American Association of Orthodontists), early orthodontic treatment improves proper jaw alignment in order to achieve a healthier bite as the face and jaws continue to grow. While younger patients, aged 7 to 10, tend to be somewhat excited about braces and the ability to change their colorful rubber bands, teenagers are less so. It’s much harder to motivate them about their orthodontic experience. I believe one reason teens are not as excited to start treatment is because there is a tendency of being disengaged from authority figures, whether it’s teachers, parents, or doctors. Second, that’s the age they are discovering themselves and becoming insecure about their external appearances. They may fear orthodontics will make them physically unattractive or change the way they speak. In addition, these patients have likely heard exaggerated horror stories from peers or even parents about orthodontic treatment, so they view it as adding to the awkwardness of being a teenager.
[sidebar float=”right” width=”275″]
Increasing Compliance Among Teen Patients
Patient compliance has long been a challenge in orthodontics, especially as it relates to treating teen patients. While it may be difficult or even frustrating evaluating the likelihood that teenagers will comply with orthodontic treatment protocols such as rubber bands, headgear, hygiene, and now accelerated treatment devices, such as AcceleDent®, I’ve identified five tips for evaluating and enhancing compliance among young orthodontic patients.
1. Parents Know Best
Ask parents if the patient is generally responsible. How many, if any, technology devices—such as smartphones, tablets, fitness trackers—have they lost and/or broken? Do they wear their glasses or do they lose them? Do they remember to do their homework, close the garage door, lock the house door, set the alarm? Having parents recall these behaviors will give you a more accurate indication about compliance.
2. Dental Hygiene Is a Good Indicator
How consistent and/or thorough is the teen at brushing their teeth? How often do the parents have to remind the teen?
3. Identify Motivation
Even if the teen doesn’t quite meet the benchmarks of #1 and #2 above, if they are motivated to complete treatment prior to 8th grade graduation, prom, senior photos, or a similar goal, they are more likely to be compliant. Once this motivation is identified, remind them of it as often as possible.
4. Tap Into Their Daily Routine
Ask the teens about their daily routine and what time they typically do their homework, watch TV, prepare for bed, etc, and have them pair that activity with the orthodontic protocol. They can even set a timer on their smartphone if they have one.
5. Have the Teens Grade Themselves
To enhance compliance, I have my teen patients grade themselves during every appointment. Using AcceleDent as an example, they are supposed to use the device 20 minutes daily, so that particular grading scale is as follows:
A = 7/7 days
C = 4/7 days
F = 0/7 days
No teen wants to be viewed as a failure or disappointment, so using a grading scale that they’re already familiar with encourages them to meet the expectations. OP[/sidebar]This is where accelerated orthodontic treatment can appeal to this population specifically. In my practice, where 70% of patients are adolescents, we have integrated AcceleDent® from Houston-based OrthoAccel Technologies Inc into our treatment protocol. AcceleDent is the first and only FDA-cleared vibratory orthodontic device. Clinically, AcceleDent has been proven to speed up orthodontic treatment by as much as 50% and relieve the discomfort often associated with treatment.1 Patients put AcceleDent in their mouth for 20 minutes daily and the device’s pulsatile forces gently accelerate tooth movement at the cellular level.
Offering AcceleDent allows me to capitalize on two factors that teenagers find appealing. One, using technology for solutions in every facet of life, and, two, the opportunity for faster gratification and results. I’ve found that once my treatment coordinator explains the AcceleDent technology to them, the teens are more motivated to participate in their orthodontic treatment. Their attitudes change because they’re excited about being able to complete treatment prior to graduation, school dances, or even college orientation.
A lightweight, easy-to-use device with a USB port for charging and usage review, AcceleDent fits within teenagers’ existing realm of technology. They use technology to complete homework, connect with friends, shop, track exercise, and identify entertainment options. For most of the teens that I prescribe AcceleDent treatment, there is not a compliance issue because we emphasize that they play an active role in speeding up their orthodontic treatment to meet whatever milestone or goal that is approaching.
Parents are very receptive to faster treatment as well because many remember their own orthodontic experience as painful and that it took too long. They, by default, have to be active in their child’s orthodontic process—taking time off work to bring their child to appointments, and reminding them about food restrictions and oral hygiene. Parents also have to endure any complaints about the associated aches and pains, and overall frustration with treatment. According to a 2014 survey of AAO members, the average length of orthodontic treatment is 22 months.2 So, if we’re reducing that time by up to half, there’s no doubt that accelerating treatment significantly reduces the parental burden that accompanies treating their children. Because of AcceleDent’s clinically proven ability to reduce the discomfort of orthodontic treatment in conjunction with self-ligating brackets, we rarely, if ever, hear of parents having to give their teens pain relievers or bringing them in for emergency pain appointments.
In my practice, I’ve eliminated the risks associated with the additional costs of accelerated orthodontics by offering a 60-day, no-risk trial of AcceleDent through OrthoAccel’s AcceleDent NOW program. For a parent, that translates into observing a teen’s compliance with AcceleDent for 60 days, and if they are not actively using the device as required, the parent returns it to my office and receives a full refund. Therefore, there is no obligation to keep the AcceleDent device. The key to this program from the outset is to simply ask the parent to give you an accurate gauge of whether or not they believe their child will be compliant.
From my perspective, faster orthodontic treatment with AcceleDent also decreases the risks associated with poor hygiene that tends to become evident among teens in prolonged orthodontic treatment. As we know, the risk of developing caries and white spot lesions increases as the length of treatment increases.3 General practitioners, who are typically orthodontists’ primary referral source, also appreciate the benefits of accelerated treatment because their patients’ teeth will be healthier over the long term.
Clinical Results
Since efficiency is a very important component of my treatment and business philosophy, I’ve been offering AcceleDent for 4 years because it gives patients the noninvasive, accelerated treatment that they want while also allowing me to achieve the quality clinical results that are important to me. The case studies of Patient 1 and Patient 2 illustrate how accelerated treatment planning can result in teeth tracking to their desired and optimal position as well as excellent jaw and chin alignment, creating good facial symmetry.


Figure 1: Patient 1 presented with a Class II dentoskeletal malocclusion with moderate overbite and erupted canines.
Patient 1, who was 12 years old when she commenced treatment, is the daughter of one of my former patients. The mother and daughter were a clear example of a parent who was empathetic to her child’s treatment because of her own treatment experience. In addition, the adolescent was motivated to comply because she wanted to complete treatment prior to beginning high school.
Patient 1 had a Class II dentoskeletal malocclusion with a moderate overbite and partially erupted canines (Figure 1). The upper right canine was high and blocked out of the arch form. Crowding was present in both maxillary and mandibular arches with a maxillary midline diastema. The treatment goal was to move the upper canines down into position while establishing a Class I molar relationship. During treatment, both arches were expanded to help resolve some of the crowding and the Carriere® Motion appliance (Henry Schein Orthodontics) with elastics was used for Class II correction and overjet reduction.


Figure 2: At finish, canines had moved down into the arch, resulting in good canine occlusion. Facial profile and balance also improved.
At the finish, you can see the canines moved down into the arch and there is good canine occlusion (Figure 2). Her facial profile and facial balance were improved as well. Retention included bonded lingual retainers on both arches with a maxillary Hawley retainer to be worn at night.
My original treatment projection for Patient 1 was 20 to 26 months, but with AcceleDent we were able to move her teeth 30% faster, completing treatment in just 18 months. With the important deadline in mind, Patient 1 was very compliant throughout treatment and was extremely satisfied that she completed treatment prior to her 8th grade graduation.

Figure 3: Treatment goals included correcting the Class II relationship, aligning both arches, and decreasing the overbite and overjet.
Patient 2 presented with a Class II malocclusion, a short lower anterior facial height, a severe overbite, moderate overjet, generalized spacing in the maxillary arch, and crowding in the mandibular arch (Figures 3 and 4). Treatment goals included correcting the Class II relationship, aligning both arches, and decreasing the overbite and overjet while improving her facial aesthetics. The midline discrepancy was not a patient or parent concern to address during the treatment and that issue was primarily due to a mild facial asymmetry.
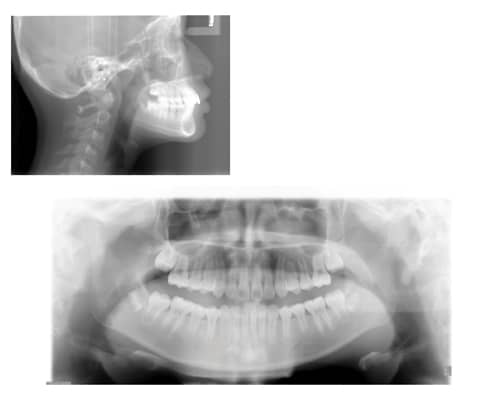
Figure 4: Initial patient scans.
She was treated with bilateral Carriere Motion appliances, fixed appliances, and elastics. She was 11 years old at start of treatment and complied with AcceleDent perfectly. I was pleased with the treatment outcome, especially with the Class II correction. Her facial balance and profile were improved as well. I projected that standard treatment for her would have taken 18 to 24 months. With AcceleDent, she accelerated her treatment and completed in just 15 months (Figure 5).

Figure 5: Patient completed treatment in 15 months using AcceleDent as part of her treatment.
My standard appointment intervals for patients are about 5 to 10 weeks, but because AcceleDent helps accelerate bone modeling and remodeling in the dentoalveolar complex, my accelerated treatment patients come in for appointments every 3 to ?5 weeks.
On average, I see about 60 to 80 patients during office hours with about 400 new case starts per year. There is not a day that passes that someone doesn’t ask me, “How much longer until I get my braces off?” That’s why I believe everybody is a candidate for accelerated treatment with AcceleDent, and it has become the standard of care for all my patients. This device really helps overcome two of the main hurdles in orthodontics: speed and discomfort. My ultimate goal is to make sure I find every possible way to start and finish a patient’s orthodontic treatment as quickly and as comfortably as possible, while achieving the results that meet high standards of quality. As a result, both the patient and practice benefit. OP?
 Mart McClellan, DDS, MS, is a Diplomate of the American Board of Orthodontics and past president of the Illinois Society of Orthodontics. Board certified in orthodontics, he practices at McClellan and Sagun Orthodontics in Kenilworth, Ill. McClellan has practiced for 23 years and has lectured nationally and internationally on strategic financial planning.
Mart McClellan, DDS, MS, is a Diplomate of the American Board of Orthodontics and past president of the Illinois Society of Orthodontics. Board certified in orthodontics, he practices at McClellan and Sagun Orthodontics in Kenilworth, Ill. McClellan has practiced for 23 years and has lectured nationally and internationally on strategic financial planning.
References
1. Cyclic loading (vibration) accelerates tooth movement in orthodontic patients: A double-blind, randomized controlled trial. Pavlin D, Anthony R, Raj V, Gakunga PT. Semin Orthod. 2015;21(3):187–194.
2. The Economics of Orthodontics. The American Association of Orthodontics. 2014.
3. Julien KC, Buschang PH, Campbell PM. Prevalence of white spot lesion formation during orthodontic treatment. Angle Orthod. 2013;83(4):641-7. doi: 10.2319/071712-584.1. Epub 2013 Jan 4.
5. Khalaf K. Factors affecting the formation, severity and location of white spot lesions during orthodontic treatment with fixed appliances. J Oral Maxillofac Res. 2014;5(1):e4. doi: 10.5037/jomr.2014.5104. eCollection 2014 Jan.
6. Richter AE, Arruda AO, Peters MC, Sohn W. Incidence of caries lesions among patients treated with comprehensive orthodontics. Am J Orthod Dentofacial Orthop. 2011;139(5):657-64. doi: 10.1016/j.ajodo.2009.06.037.
7. Wendy D. Lobre, Brent J. Callegari, Gary Gardner, Curtis M. Marsh, Anneke C. Bush, and William J. Dunn. (2015) Pain control in orthodontics using a micropulse vibration device: A randomized clinical trial. Angle Ortho. In Press.