|
| Bill Dischinger, DMD |
Orthodontic Veneer System
Bill Dischinger, DMD
Lake Oswego, Ore
Small laterals are very common in our patient population. Most of these cases can be treated with minimal changes to our normal routine. Some cases require a small amount of interproximal reduction to the lower incisors to balance out the Bolton discrepancy, and others require bonding to be placed on these small laterals, either for aesthetics or based on patient preference.
I have often found these cases to be frustrating. As we are nearing the end of treatment, I invariably ask the patient to go see his or her general dentist to evaluate the spaces I have created. If I am fortunate enough to hear back from the dentist, it is usually something along the lines of “Move number 7 0.5 mm distal while creating more space mesial. …”
We then usually go through this routine about three or more times before we finally have it just right. We then remove the braces, and the patient has ugly spaces around the laterals until they have the bonding procedure done. We then need to remake the retainers for them, hoping that they come in right away before teeth have moved slightly.
 |
 |
 |
 |
| Clockwise from top left: pretreatment, the day the veneers were placed, progress photo, and debonding day. | |
Needless to say, I wanted to find a better way of doing this. The Reliance Orthodontic Veneer System was the answer. It is so easy to use, even we orthodontists can make great-looking veneers.
If a patient has adequate space around the small laterals before treatment begins, I bond veneers the day of our initial bonding appointment. I then have perfectly sized laterals from the first day of treatment. I bond a bracket on the tooth and treat my case as I normally would for any routine treatment. If the space is not quite adequate, I place open-coil springs on both the mesial and distal of the laterals and open up space. It doesn’t matter if I open up too much space; I can always close it with c-chain. In fact, I prefer to have extra space as it makes the interproximal surfaces easier to do and I don’t need to use any matrix strips. I remove the bracket from the laterals, place the veneers using the Reliance System, rebond the brackets, and away we go.
Once we are at the end of treatment, we can remove the braces, the patient looks great, the retainers fit, and, after bleaching, the patient is ready to go see the dentist to have the final veneers done. It is a win-win-win: for us, the patient, and the general dentist.
Since incorporating this procedure into our practice, these cases have become much easier to manage and the results have been fantastic.
 |
| Art Wool, DDS |
Reverse Curved Arch Auto-Retraction
Art Wool, DDS
Wyomissing, Pa
At times, some things are so obvious that they are overlooked. Such is the case with reverse curved arches. These arches have the almost “magic” ability to be of tremendous benefit when treating extraction cases by inducing retractive force capable of moving all six anterior teeth distally in themselves and without benefit of any type of supplemental force being applied.
Now, I know this seems like nonsense, but it has proven itself to be a great treatment aid for me during years of practice. The causation is readily explainable by means of simple physical laws of inclined planes and their application by means of orthodontic appliances. I think perhaps the action of which I speak is a direct result of my edgewise training and the later introduction of Begg light wire tooth movements after taking a course in Begg appliance therapy from Milton Sims, AO, a former associate of Raymond Begg, AO, in Adelaide, Australia.
 |
 |
 |
 |
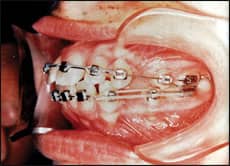
| The upper six anteriors in the upper photos show the start of the reverse curved distalization. The lower photos show the retraction achieved solely by the action of the reverse curved arch. | |
The “magic” of which I speak is readily doable in either jaw or in both simultaneously. I will, for this discussion, assume we have a bimaxillary protrusive four-bicuspid extraction case, and I will proceed with the course of care in that case. My treatment plan is to align and rotate all teeth in both jaws as quickly as possible with light, round wires and to insert a lower .018 reverse curve arch to which has been added posts for elastic hook-ups. In the upper jaw, I place an .018 reverse curved arch after all six anterior teeth have been moved into contact. This arch also has posts for elastic hook-ups, but no elastics are used initially.
I allow the reverse curved arch in the lower to protrude from the end of the buccal tubes a bit so as to prevent the tips from being caught in the buccal tubes. The action at the ends of the lower reverse curved arch is to attempt to intrude and distally rotate the lower molar. The force trying to do this is not sufficient to accomplish the movement. The arch action at the end of the buccal tube is thwarted in its effort but therein is produced a force vector that is distal in nature, along the line of the arch itself, and tends to induce a distal creep of the arch out of the buccal tube.
This distal creep is of minimal force, but quite capable over a period of time to induce the retraction of all six anterior teeth at the same time. If a light force (not to exceed 1 ounce) is added to the lower posts from a hook on the lower molar in a front-to-back configuration, the result will be a very rapid retraction of all six anterior teeth, with very minimal loss of posterior anchorage since the rotational effort exerted on the molar by the reverse curved arch is a retardant to mesial movement. Also, the toeing-in of the reverse curved arch offsets the tendency to rotate the molar.
When the lower spaces have been closed, I place heavier dimensional arches and build up the arches to the heaviest and stiffest: in my case, it would be a .021 x .025 hard steel arch. The lower arch is carried to completion and will be a guiding light for the upper dentition to occlude later in a perfect centric occlusion.
In the meantime, the upper six anterior teeth have been distally moving due to the similar action of the reverse curved arch in the upper jaw. Perhaps 1/4 to 1/3 of the total upper retraction required has been accomplished by the upper reverse curved arch all by itself. If, during any case, there is an allowable loss of some anchorage, the upper retraction may be augmented by front-to-back elastics from the posts on the reverse curved arch to the upper molar.
When the lower has been completed, the upper arch should be changed to one using less bite-opening capacity if continued bite opening is not desired. If incisor angulation is very upright and a good bit of retraction is needed, a Tri-Sectional Arch may be used, incorporating a bowing of the square posterior arch segments to augment retraction and molar stability. Class I and Class II elastic alternation is utilized to complete the upper retraction.