
By Shawn L. Miller, DMD, MMedSc
 Figure 1: Initial cephalometric radiograph.Periodontally accelerated osteogenic orthodontics (PAOO) has been an invaluable tool in our practice for many patients who in the past would have been considered orthognathic surgical candidates, or else would have been treated with significant dentoalveolar camouflage. These “borderline orthognathic surgery cases” have created almost an entire subset of patients, where PAOO is a quicker, less expensive, and less morbid treatment protocol. Therefore, in these cases, it can be argued that PAOO is a superior treatment option.
Figure 1: Initial cephalometric radiograph.Periodontally accelerated osteogenic orthodontics (PAOO) has been an invaluable tool in our practice for many patients who in the past would have been considered orthognathic surgical candidates, or else would have been treated with significant dentoalveolar camouflage. These “borderline orthognathic surgery cases” have created almost an entire subset of patients, where PAOO is a quicker, less expensive, and less morbid treatment protocol. Therefore, in these cases, it can be argued that PAOO is a superior treatment option.
We recommend PAOO for almost any patient willing to accelerate their time in braces. Certainly with the ever-increasing pace of modern society, offering 6 to 9 months of treatment duration versus 18 to 24 months is a tremendous advantage. However, beyond treating traditional orthodontic cases quicker, we found that with PAOO we could blur the line between orthognathic surgical care and traditional standard care. For many discrepancies, including Class III malocclusions, open bites, narrow arches, and some Class II malocclusions, we are able to successfully avoid orthognathic surgery while still achieving desired esthetic and functional goals.
Unfortunately, in today’s health care landscape, it has become increasingly difficult to provide treatment involving orthodontics in combination with orthognathic surgery. There are unique challenges accompanying orthognathic surgical care, all of which require more time, energy, and expense for both the doctors and patient. With increasing health care costs, especially associated hospital expenses, paying for orthognathic surgery without adequate health insurance is not feasible for many families and patients. Even if a patient has adequate medical insurance, compounding the problem is the difficulty of getting orthognathic surgical procedures approved by insurance carriers and having them deemed medically necessary. If a patient is fortunate enough to get insurance approval, in many geographic areas finding an oral and maxillofacial surgeon willing to participate with a particular insurance plan can be nearly impossible. With insurance reimbursement not keeping up with inflation and medical expenditures, many oral surgeons refuse to participate with many insurance plans, or simply may have just stopped providing orthognathic surgery.
Treatment
The surgical protocol and description of the PAOO procedure is presented elsewhere,1-3 and the biological foundation is well-reported in the literature.4-8 The PAOO is performed under intravenous sedation by trained periodontists or oral surgeons, and involves corticotomies to accelerate tooth movement and bone grafting (demineralized freeze-dried bone allografts and Bio-Oss®) to enhance bone volume after remineralization. The corticotomies can be done in localized areas of interest, or generalized to entire arches, as prescribed by the orthodontist. After sutures are placed, the patient is given prescriptions for antibiotics, Chlorohexidine rinse, and non-anti-inflammatory analgesics. Following the procedure, the patient is seen every 2 weeks for orthodontic adjustments. Treatment progress is accelerated and condensed, so frequent wire changes are necessary, elastics are given much earlier, and finishing procedures are instituted much sooner. There is approximately a 6- to 9-month window of opportunity before remineralization occurs, in which the accelerated movement subsides. Morbidity and mortality are theoretically significantly less with PAOO, particularly because general anesthesia is not necessary and a hospital stay (potential nosocomial infections) is not required.
The following are two cases, both Class III malocclusions, where we utilized PAOO to avoid orthognathic surgery.
Case 1: Eric
 Figure 2: (A) Initial maximum intercuspation occlusion. (B) Eleven months after starting treatment. (C) Follow-up photos, taken over 2 years after completing treatment.When Eric presented to our office, he was 26 years old and his chief complaint was his “underbite,” which was not only giving him functional difficulty, but also imparted cosmetic concerns. After our standard orthodontic examination and consultation, we took thorough orthodontic records, including a cone beam CT scan, mounted models, and photographs. Comprehensive functional analysis showed there was a slight shift anteriorly into maximum intercuspation, but even in a guided “centric” position, Eric was not able to get to an edge-to-edge anterior occlusion. Orthognathic surgery was presented as an option. However, for various reasons, Eric wanted to explore alternatives. Extraction of permanent teeth was another possibility. However, everyone was concerned that extractions might negatively affect his smile esthetics. We discussed PAOO for the maxillary arch as a viable option. After consulting with the oral surgeon, Eric agreed to have PAOO.
Figure 2: (A) Initial maximum intercuspation occlusion. (B) Eleven months after starting treatment. (C) Follow-up photos, taken over 2 years after completing treatment.When Eric presented to our office, he was 26 years old and his chief complaint was his “underbite,” which was not only giving him functional difficulty, but also imparted cosmetic concerns. After our standard orthodontic examination and consultation, we took thorough orthodontic records, including a cone beam CT scan, mounted models, and photographs. Comprehensive functional analysis showed there was a slight shift anteriorly into maximum intercuspation, but even in a guided “centric” position, Eric was not able to get to an edge-to-edge anterior occlusion. Orthognathic surgery was presented as an option. However, for various reasons, Eric wanted to explore alternatives. Extraction of permanent teeth was another possibility. However, everyone was concerned that extractions might negatively affect his smile esthetics. We discussed PAOO for the maxillary arch as a viable option. After consulting with the oral surgeon, Eric agreed to have PAOO.
Our diagnostic workup showed that some key issues for Eric were his dental and skeletal Class III relationships, negative overjet, posterior crossbite, mild crowding, and general misalignment (Figure 1 and Figure 2A). Some other concerns were a moderate cant (higher on left), midline discrepancy, and deep Curve of Spee. Periodontally, Eric had good oral hygiene, but had some areas with thin gingival attachment and a few areas in the beginning stages of recession. On the CT scan, thin alveolar buccal bone was noted, which is a very common finding.
 Figure 3: Follow-up cephalometric radiograph. After having full bracketing, he had maxillary arch PAOO surgery the following day. The procedure was uneventful, and we began to progress through our orthodontic treatment. Posterior light-cured glass ionomer bite ramps were used to open the bite to help with crossbite correction. Due to the severe rotation of #20, light interproximal reduction (IPR) with diamond strips was done between #20 and #21 to allow for de-rotation. After initial alignment with nickel-titanium wires, Eric was in 18×25 stainless steel wires at 12 weeks postop. A series of elastics were prescribed for full-time wear at various time points, including Class III elastics, verticals elastics, and posterior crossbite elastics. Palatal crown torque was added to the maxillary anterior archwire to control torque during the maxillary protraction.
Figure 3: Follow-up cephalometric radiograph. After having full bracketing, he had maxillary arch PAOO surgery the following day. The procedure was uneventful, and we began to progress through our orthodontic treatment. Posterior light-cured glass ionomer bite ramps were used to open the bite to help with crossbite correction. Due to the severe rotation of #20, light interproximal reduction (IPR) with diamond strips was done between #20 and #21 to allow for de-rotation. After initial alignment with nickel-titanium wires, Eric was in 18×25 stainless steel wires at 12 weeks postop. A series of elastics were prescribed for full-time wear at various time points, including Class III elastics, verticals elastics, and posterior crossbite elastics. Palatal crown torque was added to the maxillary anterior archwire to control torque during the maxillary protraction.
The occlusion and esthetics were outstanding at 9 months. However, Eric was very particular about minor cosmetic discrepancies, so an additional 2 months were spent with some very precise finishing movements. Total treatment time was therefore 11 months. A mandibular fixed retainer bonded canine to canine was given (it has since been changed to a clear vacuformed retainer), and a maxillary vacuformed retainer were given. The retainers were instructed to be worn full-time for 1 week followed by night-only wear indefinitely. Final photographs were taken at the conclusion of treatment (Figure 2B), and the follow-up records were taken 2 years after braces removal (Figure 2C and Figure 3).
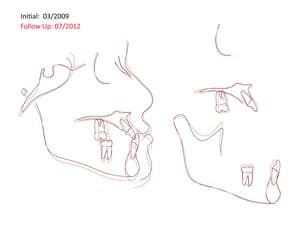 Figure 4: Superimpositions of cephalometric radiographs (initial and follow-up).Eric was pleased with his results, including the expedient nature of treatment and the fact he avoided orthognathic surgery. Overall, we were very satisfied as well. Importantly, the correction was made with good torque control of the maxillary teeth, and very little anterior flaring or tipping, which is often seen with other nonsurgical treatment modalities. The only IPR that was done was between #20 and #21. Cephalometric radiographs and analysis shows that correction was made with a combination of bite opening, maxillary dentoalveolar advancement, and mandibular dental retraction (Figure 4). (Note that there is some inherent inaccuracy in cephalometric superimpositions due to the change in alveolar shape from remodeling and bone grafting.)
Figure 4: Superimpositions of cephalometric radiographs (initial and follow-up).Eric was pleased with his results, including the expedient nature of treatment and the fact he avoided orthognathic surgery. Overall, we were very satisfied as well. Importantly, the correction was made with good torque control of the maxillary teeth, and very little anterior flaring or tipping, which is often seen with other nonsurgical treatment modalities. The only IPR that was done was between #20 and #21. Cephalometric radiographs and analysis shows that correction was made with a combination of bite opening, maxillary dentoalveolar advancement, and mandibular dental retraction (Figure 4). (Note that there is some inherent inaccuracy in cephalometric superimpositions due to the change in alveolar shape from remodeling and bone grafting.)
Case 2: Mike
Mike presented to our office as a 21-year-old young adult seeking to improve both his occlusal function and esthetics, in particular his open bite. After our standard orthodontic examination and consultation, we took thorough orthodontic records, including a cone beam CT scan, mounted models, and photographs.
 Figure 5: Initial cephalometric radiographThe diagnostic findings for Mike were his dental and skeletal Class III relationships, narrow maxillary arch with posterior crossbite, negative overjet, and high mandibular plane angle with anterior open bite (Figure 5 and 6A). Some more subtle esthetic findings included a mild cant (higher on left), midline discrepancy, dark buccal corridors, recessive lips, and inadequate tooth display upon smiling. Periodontally, Mike had good oral hygiene, but had generalized thin gingival attachment and areas with early signs of recession, although interproximal bone heights were within normal. On the CT scan, thin alveolar buccal bone was noted, similar to the first case presented.
Figure 5: Initial cephalometric radiographThe diagnostic findings for Mike were his dental and skeletal Class III relationships, narrow maxillary arch with posterior crossbite, negative overjet, and high mandibular plane angle with anterior open bite (Figure 5 and 6A). Some more subtle esthetic findings included a mild cant (higher on left), midline discrepancy, dark buccal corridors, recessive lips, and inadequate tooth display upon smiling. Periodontally, Mike had good oral hygiene, but had generalized thin gingival attachment and areas with early signs of recession, although interproximal bone heights were within normal. On the CT scan, thin alveolar buccal bone was noted, similar to the first case presented.
Our goal was to correct his Class III dental relationship and develop proper anterior guidance systems with appropriate overjet and overbite. Esthetically, we felt it was equally important to enhance his smile by broadening the upper arch, improving lip support, and providing more tooth display upon smiling. We did not want to camouflage by retracting lower anteriors via temporary anchorage devices, IPR, and/or extractions. Minimizing the length of time in treatment was also an important consideration for Mike. Therefore, we developed a plan centered on PAOO for the maxillary arch, with the caveat that if we were unsuccessful attaining our goals, orthognathic surgery would be utilized for final correction.
 Figure 6: (A) Photos show initial occlusion. (B) Final photos, 8 months after starting treatment. (C) Follow-up photos, 1 year after completing treatment.Full bracketing was done, and the following day PAOO was performed according to standard protocols on the maxillary arch only. At 4 weeks postop, a rapid alveolar expander (RAE) was delivered and activated once per day for 4 weeks to expand the maxillary alveolus. With PAOO, there is no mid-palatal sutural expansion; it is purely dentoalveolar expansion. During this expansion period, a reverse-pull headgear was also used 10 to 12 hours per day with increasing elastic forces over a period of 6 weeks. Although somewhat unorthodox in adults, the reverse-headgear was something Mike was willing to wear for a short period in order to avoid orthognathic surgery. Similar to the RAE, the headgear provides maxillary dentoalveolar protraction, not true skeletal protraction. The RAE was removed approximately 14 weeks postop. For the next 4.5 months we continued our orthodontic archwire sequence, including Class III elastics and vertical finishing elastics. At 8 months postop, Mike was completed with treatment. The braces were debonded, and we delivered upper and lower vacuformed retainer appliances. Retainers were worn full-time for 1 week followed by night-only wear only indefinitely.
Figure 6: (A) Photos show initial occlusion. (B) Final photos, 8 months after starting treatment. (C) Follow-up photos, 1 year after completing treatment.Full bracketing was done, and the following day PAOO was performed according to standard protocols on the maxillary arch only. At 4 weeks postop, a rapid alveolar expander (RAE) was delivered and activated once per day for 4 weeks to expand the maxillary alveolus. With PAOO, there is no mid-palatal sutural expansion; it is purely dentoalveolar expansion. During this expansion period, a reverse-pull headgear was also used 10 to 12 hours per day with increasing elastic forces over a period of 6 weeks. Although somewhat unorthodox in adults, the reverse-headgear was something Mike was willing to wear for a short period in order to avoid orthognathic surgery. Similar to the RAE, the headgear provides maxillary dentoalveolar protraction, not true skeletal protraction. The RAE was removed approximately 14 weeks postop. For the next 4.5 months we continued our orthodontic archwire sequence, including Class III elastics and vertical finishing elastics. At 8 months postop, Mike was completed with treatment. The braces were debonded, and we delivered upper and lower vacuformed retainer appliances. Retainers were worn full-time for 1 week followed by night-only wear only indefinitely.
 Figure 7: Follow-up cephalometric radiographFinal photographs were taken at the conclusion of treatment (Figure 6B) and follow-up records at 1 year post-treatment (Figure 6C). We were quite satisfied with the stability and periodontal health. The functional occlusion and anterior guidance systems have been maintained. The esthetics were much improved, including the smile arc, arch width, and buccal corridors. There is slight improvement to the cant (it was not one of our treatment goals to correct it). Torque control of the maxillary anterior teeth was very good. Cephalometric radiographs and analysis shows similar findings to the first case presented. Correction was made with a combination of bite opening, maxillary dentoalveolar advancement, and mandibular dental retraction (Figure 7 and Figure 8). No IPR was necessary.
Figure 7: Follow-up cephalometric radiographFinal photographs were taken at the conclusion of treatment (Figure 6B) and follow-up records at 1 year post-treatment (Figure 6C). We were quite satisfied with the stability and periodontal health. The functional occlusion and anterior guidance systems have been maintained. The esthetics were much improved, including the smile arc, arch width, and buccal corridors. There is slight improvement to the cant (it was not one of our treatment goals to correct it). Torque control of the maxillary anterior teeth was very good. Cephalometric radiographs and analysis shows similar findings to the first case presented. Correction was made with a combination of bite opening, maxillary dentoalveolar advancement, and mandibular dental retraction (Figure 7 and Figure 8). No IPR was necessary.
Conclusion
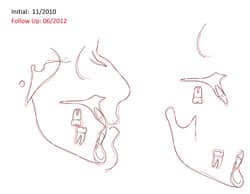 Figure 8: Figure 5: Superimpositions of cephalometric radiographs (initial and follow-up).Over the years, we have expanded our use of PAOO to more difficult and complicated cases, with more extreme malocclusions. With each successful case, we continue to stretch the boundaries of the “envelope of orthodontic movement” while still providing stable and periodontally sound treatment. There has not yet been a conclusive research study that has clearly defined the outer limits of PAOO for mandibular or maxillary dentoalveolar changes. The accelerated movement is of tremendous benefit to the patient, but is not where the true potential of PAOO lies. In our practice, PAOO is redefining surgical orthodontics, and we are excited to continue to utilize the procedure as an integral part of our practice to provide exceptional care. OP
Figure 8: Figure 5: Superimpositions of cephalometric radiographs (initial and follow-up).Over the years, we have expanded our use of PAOO to more difficult and complicated cases, with more extreme malocclusions. With each successful case, we continue to stretch the boundaries of the “envelope of orthodontic movement” while still providing stable and periodontally sound treatment. There has not yet been a conclusive research study that has clearly defined the outer limits of PAOO for mandibular or maxillary dentoalveolar changes. The accelerated movement is of tremendous benefit to the patient, but is not where the true potential of PAOO lies. In our practice, PAOO is redefining surgical orthodontics, and we are excited to continue to utilize the procedure as an integral part of our practice to provide exceptional care. OP
References
1. Ferguson DJ, Wilcko WM, Wilcko MT. 2006. Selective alveolar decortication for rapid surgical-orthodontic resolution of skeletal malocclusion. In: Bell WE and Guerrero C, eds. Distraction Osteogenesis of the Facial Skeleton. Hamilton, Ontario, Canada: BC Decker.
2. Wilcko WM, Ferguson DJ, Bouquot JE, Wilcko MT. Rapid orthodontic decrowding with alveolar augmentation: case report. World J Orthod. 2003;4:197-205.
3. Wilcko MT, Wilcko WM, Bissada NF. An evidence-based analysis of periodontally accelerated orthodontic and osteogenic techniques: a synthesis of scientific perspectives. Seminars in Orthodontics. 2008;21(4):305-316.
4. Frost HA. The regional acceleratory phenomena: a review. Henry Ford Hosp Med J. 1983;31:3-9.
5. Gantes B, Rathburn E, Anholm M. Effects on the periodontium following corticotomy-facilitated orthodontics. J Periodontol. 1990;61:234-238.
6. Twaddle BA, Ferguson DJ, Wilcko WM, Wilcko MT, Lin CY. Dento-alveolar bone density changes following accelerated orthodontics. J Dental Res. 2002;80:301.
7. Yaffe A, Fine N, Bindermen I. Regional accelerated phenomenon in the mandible following mucoperiosteal flap surgery. J Periodontol. 1994;65:79-83.
8. Lino S, Sakoda S, Ito G, Nishimori T, Ikeda T, Ikyawaki S. Acceleration of orthodontic tooth movement by alveolar corticotomy in the dog. Am J Orthod Dentofacial Orthop. 2007;131:448.e l-8.
 |
Shawn L. Miller, DMD, MMedSc, is in private practice in Orange and Aliso Viejo, Calif. He completed his dental degree at the University of Pennsylvania and his Masters of Medical Sciences and orthodontic residency at Harvard University. He lectures locally on PAOO, Incognito, and Interdisciplinary Orthodontic Treatment. He is Board Certified by the American Board of Orthodontics. He can be reached at [email protected]. |








