
by Lital von zur MÜhlen, Dr Med Dent, and Dirk Wiechmann, Dr Med Dent
Class II correction using a customized lingual appliance system with a Herbst device
-

- Lital von zur MÜhlen,
Dr Med Dent

-

- Dirk Wiechmann,
Dr Med Dent

The Herbst device has gained popularity in the last 20 years and is for many orthodontists the appliance of choice for the treatment of Class II malocclusions. One major benefit of the Herbst device is that, unlike headgear, its effectiveness is not determined by patient compliance, and clinical studies have shown that Herbst therapy is successful in both mixed and permanent dentition.1 In addition, the Herbst device’s effects on mandibular length have been shown to be significant when used on older patients. According to Hans Pancherz, Dr Med Dent; and Sabine Ruf, Dr Med Dent, from the University of Geisen, the Herbst can be used effectively to treat both adolescents and young adults.2,3
Patient demand for invisible orthodontics has increased dramatically in the last 7 years. More patients are aware that invisible treatment is an option because of advertising campaigns for aligners and television programs that show patients getting dental makeovers. Recent studies linking oral health to overall health have been widely publicized. Adults seek orthodontic treatment to both change their appearance and take advantages of the health benefits of straight teeth.
Lingual Orthodontics
Lingual orthodontic treatment has always been popular in Europe and Asia. It is the preferred treatment choice for patients with aesthetic concerns. Orthodontists who wish to offer invisible treatment to their patients prefer a fixed appliance because it offers them complete control and is extremely flexible.
Lingual orthodontics has not been as popular in the United States because in the past it was more difficult to learn, required significantly more chairtime, and was very uncomfortable for patients. The original lingual technique was introduced almost 30 years ago. Treating patients with a traditional, noncustomized lingual appliance is clinically challenging for the following reasons: 1) the lingual surface of the teeth are anomalous, making bracket placement, bracket adhesion, and bracket rebonding more difficult; 2) interbracket distances are shorter, making the mechanics less efficient; 3) bending is reversed, making wire-bending challenging; and 4) predictable finishing is problematic due to imprecise slot geometry.
In the last 5 years lingual orthodontics has experienced a resurgence in the United States and Canada due to the introduction of a new 100% customized system that solves many of the issues associated with older lingual systems. The driving concept behind iBraces is putting as much intelligence into the appliance as possible to minimize doctor time and deliver predictable clinical results.
Using iBraces, brackets do not need to be repositioned and the orthodontist does not bend wires during treatment. Brackets are delivered in an indirect bonding tray so that bracket placement is simplified and correct from the beginning of treatment. A sequence of customized archwires is created in the laboratory to deliver the results specified in the individual target setup.
The system is designed for patient comfort and is more attractive to patients than older, noncustomized appliance systems. Doctors and patients who earlier would not have considered lingual orthodontics as a treatment option are trying this new system.
One major benefit of lingual orthodontic treatment over aligner therapy is that, as with Herbst therapy, treatment success is not dependent on patient compliance. The appliance is fixed and cannot be removed by the patient. This gives the orthodontist much greater control over the treatment and the final result.
Herbst Therapy and Lingual Orthodontic Treatment
Very little literature is available regarding the use of the Herbst device in conjunction with lingual orthodontic treatment. One goal of this article is to demonstrate the advantages of combining these two techniques. Using a Herbst device with a precise, customized lingual appliance system has many benefits to both the orthodontist and the patient, the most clinically relevant of which is controlling proclination of the lower incisors during treatment.
The lingual orthodontic appliances I use are designed using CAD/CAM software and manufactured using advanced mass-customization techniques. The process starts with the orthodontist submitting an impression. The impression is used to create a therapeutic setup, which is scanned into a computer. Then the appliance is designed.
Benefits of Combining the Herbst Device with a Customized Lingual System
-

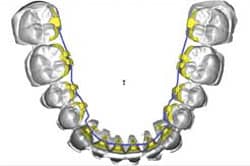
- Figure 1: As part of the design process, the Herbst device is modeled on the computer.

As part of the overall appliance design and manufacturing process, the orientation of the Herbst device is modeled in the computer (Figure 1) The Herbst device consists of a bilateral telescope mechanism attached between lower and upper dental arches to retain the mandible in a continuous anterior position. The bracket base of the upper first molar and lower canine extends to the labial surface and supports the pivots for the Herbst telescopes. The bracket base and the pivot base are designed and manufactured as a single unit to prevent breakage between the two components.
Designing the Herbst device in the computer as a part of a completely customized system has two major advantages. First, it is possible to check that the pivot position on the molar and the lower canine is perpendicular to the Herbst device to ensure proper alignment and reduce binding and breakage once it is placed in the patient’s mouth. Second, the bracket slots and wire geometry of the customized lingual appliance are extremely precise, enabling the orthodontist to control proclination of the incisors, a common side effect of Herbst therapy.
Patient Treatment with a Herbst and a Customized Lingual System
When an orthodontist intends to use a Herbst with the customized lingual system, the orthodontist must indicate on the laboratory form that a Herbst device will be used for Class II correction. The lab will set up the teeth to a Class I situation. The orthodontist must also indicate on the laboratory form the position of the lower incisors: whether they should be proclined, kept in their current position, or uprighted.
-

- Figure 2: Molar bands are designed with labial attachments.

Molar bands with labial attachments are designed for placement at the beginning of treatment, along with two sets of canine brackets. (Figure 2) A regular set of canine brackets is used during the leveling and alignment phase of treatment. After leveling and alignment, the regular canine brackets are removed and replaced with Herbst series brackets.
Sample Patient
Diagnosis: A male adolescent patient with Class II malocclusion, moderate crowding, deep bite, and amelogenesis imperfecta.
Treatment Plan: Due to the patient’s amelogenesis imperfecta, a lingual appliance was used to prevent further decalcification of the labial tooth surfaces. The goal was to correct the moderate crowding and align both arches with fixed lingual therapy and compensate Class II with a Herbst device. Canine brackets with bite planes were used to aid in opening the bite.
-
- Figure 3: The patient had severe labial decalcification and slight lingual decalcification.

Archwire Sequence:
- 0.016-inch round SE NiTi
- 0.018- x 0.025-inch SE NiTi
- 0.018- x 0.025-inch stainless steel
Initial Photos (Figure 3): Notice that the lingual tooth surfaces have only slight decalcification.
Bonding the Lingual Appliance: The lower arch was bonded first, and double overties were used to ligate anterior brackets. The upper arch was bonded 2 weeks later. Note that the molar brackets have the Herbst attachments. Molar bands do not go interproximal—they go around the occlusal surface. As a result, it was not necessary to create space prior to bonding the bands. Light, round SE NiTi (0.016-inch) wires were placed for initial leveling and alignment.
-
- Figure 4: After 3 months, NiTi wires and Herbst series wires were placed.

The decision to bond one arch at a time is based on an assessment of the patient’s ability to adapt to the appliance. In cases where the orthodontist believes that the patient may have an issue adapting to the appliance, it is better to bond one arch at a time. In this situation it is recommended to bond the lower arch first.
Second Wire (Figure 4): After 3 months, full-sized (0.018- x 0.025-inch) SE NiTi wires were placed in preparation for the insertion of the full-sized stainless steel wires that will be used during Herbst therapy. The Herbst series canine brackets were placed at this time.
Third Wire (Figure 5): The full-sized stainless steel (18 x 25) wire was engaged. One month later, the Herbst therapy began. Note the slight overcorrection of the Class II. The treatment result matches the setup in the computer.
-
- Figure 5: A month after an 18 x 25 stainless steel wire is engaged, the Herbst appliance is placed. Note the overcorrection of the Class II.

-
- Figure 6: After 14 months of treatment, the objectives have been met with no further tooth damage.

Final Photos (Figure 6): After 14 months of comprehensive treatment, all treatment objectives have been met. No further damage is evident on the lingual or labial tooth surfaces.
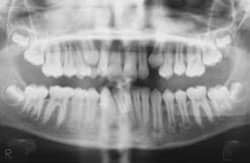
X-rays reveal that the roots are parallel at the end of treatment and proclination of the lower incisors was prevented. The precise wire geometry and slot dimension provided superior torque control of the lower incisors during Herbst treatment.
 |
 |
| Before treatment, the labial surfaces of the teeth show some decalcification. | A clear view of the lingual appliance. |
 |
 |
| The treatment result matches the setup in the computer. | After treatment, no further damage is visible on the labial surfaces. |
 |
 |
 |
|
| Post-treatment x-rays show that the roots are parallel and that proclination of the lower incisors was prevented. |
Lital von zur MÜhlen, Dr Med Dent, is an orthodontist with private practices in Hamburg and DÜsseldorf, Germany. She is a member of the original clinical group that developed the customized lingual technique. Since November 2001, she has treated more than 300 patients using this technique. She is a clinical adviser for Lingualcare.
Dirk Wiechmann, Dr Med Dent, is the principal inventor of the first completely customized lingual bracket system, iBraces/Incognito. He has published numerous articles in scientific journals related to lingual orthodontics and spoken at conferences worldwide. In his private practice in Bad Essen, Germany, he has more than 300 lingual patients in active treatment. He is a faculty member at the Medical School, Hannover, Germany and the Scientific Director of the postgraduate program in lingual orthodontics at the University of Paris VII, France. Since 2006 he has been honorary associate professor of dentistry at the University of Hong Kong, China.
References
- de Almeida MR, Henriques JFC, de Almeida RR, Weber D, McNamara JAJ. Short-term treatment effects produced by the Herbst appliance in the mixed dentition. Angle Orthod. 2005;75(4):540-547.
- Ruf S. Optimal time for treatment with the Herbst appliance. Orthod Fr. 2006;77:163-167.
- Pancherz H. The Herbst appliance: its biologic effects and clinical use. Am J Orthod. 1985;87:1-20.








