
by Kevin C. Walde, DDS, MS
Using the easy molar distalizer for maxillary molar distalization
 Distalizing maxillary first molars is often an objective in treatment plans involving Class II malocclusions, and it is sometimes indicated for nonextraction treatments with maxillary crowding. The increasing lack of patient compliance has become a factor in choosing effective orthodontic appliances for molar distalization. In recent years, various appliances that do not require patient compliance have been developed to drive maxillary molars distally.1–5
Distalizing maxillary first molars is often an objective in treatment plans involving Class II malocclusions, and it is sometimes indicated for nonextraction treatments with maxillary crowding. The increasing lack of patient compliance has become a factor in choosing effective orthodontic appliances for molar distalization. In recent years, various appliances that do not require patient compliance have been developed to drive maxillary molars distally.1–5
All of these appliances have demonstrated their ability to distalize maxillary first molars. Some of these appliances, however, produce unwanted tipping of the maxillary molars.5 One of them has a tendency to create crossbites. They vary in how difficult they are to fabricate, deliver to the patient, and activate following delivery of the appliance.
This article describes a new, easy-to-fabricate and easy-to-use noncompliance appliance for molar distalization*. It was developed to produce little or no molar tipping. Fabrication and delivery are relatively simple, and, true to its name, the easy molar distalizer is very easy to activate.
Like the appliances mentioned above, the easy molar distalizer uses a modified Nance button banded or bonded to premolars or primary molars as an anchor unit (Figure 1). It is easily activated from the anterior by simply turning the screw counterclockwise (Figure 2). Additionally, the distalizing spring can be removed and adjusted, if desired.

The manufacturer supplies the appliance as three pieces: 1) the main body; 2) the universal distal spring or legs (made from .032-inch stainless steel); and 3) an activation tool (Figure 3). This appliance can be constructed by any commercial orthodontic laboratory, or the parts can be provided for construction by in-house laboratories.
First molars bands with lingual sheaths are cemented in the patient’s mouth. (Alternatively, the first molars bands can be cemented at the time the appliance is delivered to the patient.)
An alginate impression is taken, with particular attention being given to the detail of the palate, the occlusal and lingual surfaces of the teeth, and the lingual sheaths of the molar bands. A model is made from laboratory stone, and anchor wires are bent from .028-inch round stainless steel to attach the anchor teeth to the Nance button. These wires work best when they lie in the embrasures distal to the anchor teeth. We have used anchor wires soldered to premolar bands for anchorage, but doing so makes the appliance more difficult to construct.
A Nance button is fabricated to cover a large portion of the palate. Anterior extensions are embedded in the acrylic, locking the appliance securely in place. The appliance should be positioned anteroposteriorly so that the distal is flush with the mesial aspect of the lingual sheaths on the first molar bands. Occlusoapically, it should be positioned at approximately the trifurcation of the maxillary first molars. This is usually 10 to 12 mm from the occlusal surface (Figure 4, page 26). This will place the appliance at approximately the center of resistance of the molars for bodily tooth movement. Occlusoapical positioning is critical! If the appliance is placed too far occlusally, more crown tipping will occur; if it is placed too far apically, more root tipping will occur. The body of the appliance can be removed from the acrylic for easier polishing (Figure 5A and 5B).
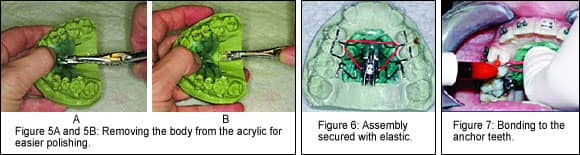
The “legs” of the appliance are fabricated from a .032-inch stainless-steel wire. Double back bends are made to insert into lingual sheaths on the maxillary first molar bands. Loops are provided bilaterally for fine-tuning adjustments before insertion or during use. The midportion of the spring is inserted into a slot in the distal of the appliance, and the assembly is secured with an elastic to be delivered to the patient (Figure 6).
 Patient Delivery
Patient Delivery
The lateral ends of the spring are inserted into the lingual sheaths on the molar bands. The Nance button is held firmly in place against the palate with finger pressure. The appliance is then bonded to the anchor teeth (Figure 7).
Activation
The appliance is activated with a tool that is inserted from the anterior into the head of the screw and rotated counterclockwise (Figure 2, page 26). Each 360º turn activates the appliance 0.4 mm. Three to five full turns per appointment are effective. Activation takes a matter of seconds. Appointments are made at 4- to 8-week intervals, depending on the amount of activation applied and on operator preference. If it is necessary to adjust the spring, a three-pronged plier can be used or the spring can be loosened by backing up the screw. Securing the spring with floss is recommended to prevent accidental aspiration. Molar distalization takes 4 to 8 months, depending on the amount of distalization required. Once the desired degree of distalization is achieved, the screw should be sealed with composite resin or acrylic to prevent backup.
The premolars, canines, and incisors are then retracted sequentially. Molar distalization is maintained by using a stopped archwire with support from Class II elastics. If Class II elastics cannot or will not be used, some sort of auxiliary appliance (such as Forsus or Jasper Jumper) should be used.
It has been my preference and suggestion to align the maxillary arch to the extent possible with a full-sized archwire to augment the anchorage provided by the Nance button. The archwire is then sectioned mesial to the maxillary first molars with the rest of the dental arch, providing additional anchorage. However, Bowman,6 in a presentation given at the AAO Annual Session in Las Vegas, suggested that it may be advantageous to use anchor teeth that have not been orthodonticallymobilized when using molar-distalizing appliances. His suggestion is based on studies of the effect of molar distalizers (particularly the Distal-Jet) on anterior anchorage. These finding may be applicable to the easy molar distalizer as well.


The introduction of mini-implants for anchorage could provide interesting possibilities for future applications.
|
Case Selection
The easy molar distalizer can be used almost any time maxillary first molar distalization is required. It can be used bilaterally or unilaterally for correcting Class II molar relationships or for relieving maxillary crowding when nonextraction treatment is desirable. It can also be used for distalization in first-phase orthodontics or for single-phase orthodontics in combination with fixed appliances.
Kevin C. Walde, DDS, MS, is in private practice in Washington, Mo, and is an assistant clinical professor in the Department of Graduate Orthodontics at St Louis University. He is a member of the AAO, a Diplomate of the American Board of Orthodontics, past president of the Greater St Louis Orthodontic Study Club, and a past president of the Orthodontic Education and Research Foundation.He can be reached via e-mail at [email protected].
*U.S. Patent No. US 6,435,870
References
1. Gianelly AA, Vaitas AS, Thomas WM, Berger DG. Distalization of molars with repelling magnets. J Clin Orthod. 1988;22:40–44.
2. Jones RD, White JM. Rapid Class II molar correction with an open-coil jig. J Clin Orthod. 1992;26:661–664.
3. Hilgers JJ. The pendulum appliance for Class II non-compliance therapy. J Clin Orthod. 1992;26: 706–714.
4. Carano A, Testa M. The distal jet for upper molar distalization. J Clin Orthod. 1996;30:374–380.
5. Keles A, Sayinsa K. A new approach in maxillary molar distalization: intraoral bodily molar distalizer. Am J Orthod Dentofacial Orthop. 2000;117:39–48.
6. Bowman SJ. Comments from: Molar distalization: bad English, good practice. Paper presented at: AAO Annual Session; May 9, 2006; Las Vegas, Nev.
7. Walde KC. The simplified molar distalizer. J Clin Orthod. 2003;37: 616–619.








