
by J. Clifton Alexander, DDS, MS
Ten tips for switching from labial to lingual orthodontics
 Orthodontics has gone through, and will continue to experience, dramatic changes due to technology. Most recently, there is CAD/CAM technology that allows companies to make customized brackets, both labial and lingual, as well as archwires that are robotically bent to an ideal, target occlusion based on a ideal setup. Of course, we also have the removable aligners that most of use to different degrees.
Orthodontics has gone through, and will continue to experience, dramatic changes due to technology. Most recently, there is CAD/CAM technology that allows companies to make customized brackets, both labial and lingual, as well as archwires that are robotically bent to an ideal, target occlusion based on a ideal setup. Of course, we also have the removable aligners that most of use to different degrees.
Lingual orthodontics has also gone through striking changes in recent years. Several new bracket designs have surfaced, including an entire system of 100% customized brackets along with customized, robotically bent wires. With lingual appliances, the decreased interbracket distance and the difficulty of manually bending archwires has made the technique difficult at best. Never has there been a greater need filled in lingual orthodontics than with robotically bent wires based on a final setup of the finished result.
Regardless of what type of lingual appliance you use, here are 10 tips that can be very helpful when adding lingual therapy to your practice.
1) Case Selection
When you start a new procedure or try a new appliance, it is always best to carefully choose the patient that you will “experiment” with. When I do this, I am very upfront with the patient, telling him or her that I am going to try something new, and that it holds great promise. I also usually give my very first patient a significant discount for being my guinea pig, saying, “We will learn together.”
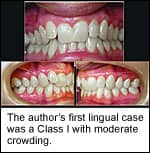
In terms of the specific patient, there are two main areas of consideration when choosing your first lingual patient. The first is the difficulty of the case. I always highly recommend orthodontists to start their first lingual case on a Class I, minor-to-moderate crowding, nonextraction case—one that might qualify for removable aligners, for example. If a patient comes to my office requesting aligners, but I feel like there is just too much to be done, I thoroughly explain the need for full control of each individual tooth with a fixed appliance and the ability the fixed appliances give me to get the teeth straight and the bite right. Otherwise, I explain, we would both be frustrated and disappointed.
The second consideration when choosing a patient is personality. It is best to have a more laid-back, go-with-the flow type than a high-maintenance, Type A person. You want a patient who is willing to let you play with the system, learning as you go, while not losing confidence in you or the system. Proper communication at the beginning is critical for this. Also, a more relaxed individual will not lose his or her patience during the course of treatment.
2) Obtain Proper Training
There is no question that there is a definite learning curve in going from labial to lingual. There are, however, several training opportunities and courses that can help you get started. There are expert clinicians who offer courses in their offices that include 2 to 3 days of training, with the opportunity to actually see live patients being treated. The company that produces the system I use has exceptional training, both initial and continuous. Orthodontists have hailed it as critical in the success of climbing that learning curve and making it fun and exciting.
You can choose between live and online training to get the orthodontist/staff introduced and certified with the system, and multiple continuous-training options are available as well. The most valued among those that use it is the on-site training by a clinical assistant who will assist the orthodontist with the initial bonding and archwire insertion, and will train the staff during the process.
3) Take it Slowly and Involve Your Staff
The first few cases will take a little longer than normal simply because you and the staff are progressing through a learning curve. Schedule your first few lingual patients at slower times of the day so that you can create a nice, fun, and relaxed atmosphere in which to treat and to learn. Patients will appreciate this. They will be the center of attention and will feel totally taken care of. Even though you’ll want to plan on slightly longer appointments for your first few patients, the overall treatment time should not be significantly affected, since you will be very attentive and efficient with these cases. The longest appointments will be the initial bonding—maybe 1 to 1.5 hours until you get the process down, then only 45 to 60 minutes. Archwire changes should not take more than 20 to 30 minutes if you’ve properly let the previous archwire work until it is fully ligated and passive. Most of the time, routine adjustments between archwire changes are very short and easy appointments for the office and the patient.
Most of the practices that I see that have successfully integrated lingual orthodontics have involved their staff from the very beginning. Of course, it is imperative that the orthodontist be the most familiar and comfortable with the techniques and procedures, but a well-trained assistant and front-office staff are key. The orthodontist will eventually rely on the assistants to be just as comfortable with routine adjustments, such as archwire changes, as they are with the labial technique. The orthodontist will need to count on accurate communication from the front desk about the differences and advantages of the appliance when asked by patients on the phone or in the office. Offices that have staff that are trainedat the same time as the orthodontist have the most success, and the most fun, with lingual orthodontics.
4) Patient Education
The new-patient exam is when relationships, trust, and rapport are initiated. It is also a critical time for patient education. In my office, after I make the initial diagnosis and present the treatment plan to the patient, I explain what types of appliances will get us to the goal line.
 If a patient has come with removable aligners on his or her mind but doesn’t qualify for that type of treatment modality, then I explain to him or her that there is less control with those than with fixed appliances, and that we want to get it right the first time. I then proceed to explain and discuss the fixed appliances. I first show him or her two typodonts—one with metal labial brackets and another with clear labial brackets. I explain the slight differences between the two, and talk about immediate oral-hygiene issues (unknown food particles between the brackets after a meal) and temporary soft-tissue irritation.
If a patient has come with removable aligners on his or her mind but doesn’t qualify for that type of treatment modality, then I explain to him or her that there is less control with those than with fixed appliances, and that we want to get it right the first time. I then proceed to explain and discuss the fixed appliances. I first show him or her two typodonts—one with metal labial brackets and another with clear labial brackets. I explain the slight differences between the two, and talk about immediate oral-hygiene issues (unknown food particles between the brackets after a meal) and temporary soft-tissue irritation.
Then, I take the third typodont off the shelf, with my lingual brackets, and say, “Now, if you want all of the same benefits of those other two but with an appliance that is 100% invisible, you could have these.” Then I open the typodont to reveal the lingual appliances. In my office, I use brackets that are cast in gold and are very small. In describing the appliance to patients, I tell them about the technology behind it and also warn them about minor, temporary tongue irritation. It is very important that patients know both facts. The understanding of the technology, individuality, and customization gives the appliance value to them, so that when the treatment coordinator tells them the fee, they are not surprised, unless it is actually less than they thought—which does happen!
 The information about possible tongue irritation and speech interferences is critical. I tell him or her that he or she may or may not have any problem, since everyone is different; but in the worst case, just give it 2 weeks and he or she will be over the hump. Some patients report absolutely no problem at all, and some take the full 2 weeks. They all eventually say it would not have kept them from having lingual appliances and would do it again because of how their teeth “magically” straightened.
The information about possible tongue irritation and speech interferences is critical. I tell him or her that he or she may or may not have any problem, since everyone is different; but in the worst case, just give it 2 weeks and he or she will be over the hump. Some patients report absolutely no problem at all, and some take the full 2 weeks. They all eventually say it would not have kept them from having lingual appliances and would do it again because of how their teeth “magically” straightened.
5) Use Recommended Setup/Bonding Procedures
Proper bracket positioning is paramount with any orthodontic appliance, even more so in lingual orthodontics, since wire bending, which results when brackets are not in their ideal position, is so difficult with the decreased interbracket space. Our goal is to achieve ideal bracket positioning so that we can let the archwires do the work. It is also very important that, should a bracket come off during treatment for whatever reason, it can be placed back in its original position accurately.
Given the fact that the lingual surface of the dentition is much more variable in our patient population than the labial surface, mass-produced brackets with prescriptions for tip, torque, and rotation values cannot be produced that fit flush to the tooth with a low profile. Rather, most standard lingual brackets have the prescription built into a custom composite pad but include very little of the lingual anatomy. The appliance I use covers a majority of the lingual surface, fitting the flush gold pad exactly to the tooth. Not only does it precisely fit the anatomy of the tooth with no custom pad, but if one comes off during treatment, it is very easy to place it back in its original position accurately. This preserves the prescription and avoids the need to bend wire.
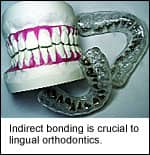
To easily and accurately place the brackets at the initial bonding appointment, it is, I believe, mandatory to use an indirect bonding procedure along with a pretreatment diagnostic setup of the case to the end-treatment objective. In this lab technique, the orthodontist prescribes the treatment objective and a lab technician resets the malocclusion models to the requested position, places the brackets on the teeth with a composite material, then transfers the brackets from the ideal setup to the maloccluded models for indirect bonding trays to be fabricated. Whether the orthodontist uses the more advanced 100% customized system of brackets and wires, or the standard brackets alone, it is important to use an indirect bonding procedure to accurately bond them.
6) Use the Recommended Armamentarium
While it is possible to immediately start treating with lingual appliances using the same instruments you use for your labial appliance, there are certainly several tools and instruments that make it easier. My staff and I very much appreciated a heavy, double-ended ligature director with a rectangular slot. This instrument is used to not only tuck metal ligatures, but also to direct and torque the archwires into the slots. One end is straight, the other is bent. Another instrument that is a great help in lingual orthodontics is a double-sided pliers that permanently bends any archwire, even the smallest nitinol wires, to a 90º angle. In lingual therapy, we often cinch back the wire distal to the terminal molar for two reasons: to keep the smaller, initial wires from slipping out of the tubes, and, most importantly, for comfort. If the smallest length of wire slides distally after being cut flush, it is a significant irritation to the tongue. If, however, the wire is intentionally left long by approximately 5 mm and is then cinched back, the wire is free to move with no consequence to the tongue.
Other instruments are useful as well; however, they are sometimes specific to the exact lingual appliance you choose. Proper training will include recommendations of other tools and instruments.
7) Appreciate the Biomechanical Differences
Based on an accurate diagnosis and treatment plan, you will be able to switch from labial to lingual orthodontics without too much thought of biomechanics in the very beginning. The main focus for the entire team will be to get through the learning curve of initial bondings, ligations, and archwire changes.
 During the course of treatment, however, you will begin to see different effects that are important to consider from a biomechanical perspective. For instance, take into consideration the point of force application. The center of resistance of the tooth will be closer to the point of force application when brackets are placed on the lingual surface of the tooth, thus providing more efficient—and many times quicker—tooth movement. In deep-bite cases like Class II, Division II malocclusions, the maxillary anterior brackets serve as a bite plane, opening the posterior segments. This simple feature proves valuable in opening the bite and leveling the lower arch much more quickly than you can with labial brackets, and without unintended bracket interferences and failures. The depth of the differences of labial to lingual biomechanics is beyond the scope of this article, but there are two reference books that go into detail on the subject.1-2
During the course of treatment, however, you will begin to see different effects that are important to consider from a biomechanical perspective. For instance, take into consideration the point of force application. The center of resistance of the tooth will be closer to the point of force application when brackets are placed on the lingual surface of the tooth, thus providing more efficient—and many times quicker—tooth movement. In deep-bite cases like Class II, Division II malocclusions, the maxillary anterior brackets serve as a bite plane, opening the posterior segments. This simple feature proves valuable in opening the bite and leveling the lower arch much more quickly than you can with labial brackets, and without unintended bracket interferences and failures. The depth of the differences of labial to lingual biomechanics is beyond the scope of this article, but there are two reference books that go into detail on the subject.1-2
 8) Be Prepared for Patient Patience
8) Be Prepared for Patient Patience
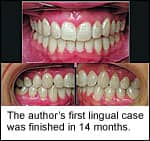
One of the most liberating aspects of the new lingual appliance I have been using for the past 3 years is the improved tolerance from the patient. In the past, the lingual appliances were necessarily larger in profile, because of the prescribed custom pad, causing significant speech and comfort issues. Despite the fact that they were invisible, the patients, predominately adults, were as anxious to have them removed as if they were labial appliances. However, with the new smaller, 100% customized appliance, the speech and comfort has so vastly improved that, if I make the comment that we are getting close, patients routinely tell me to take as long as I need to finish. They almost never pressure me to take them off. How great is that?
While I never let patients dictate treatment or pressure me to take appliances off too soon, it is an everyday occurrence that patients pester us and our staff with the questions, “How much longer?” or “When do I get these things off?” It is a welcome change when patients actually appreciate your work and commitment to getting the job done right within a well-estimated time frame. It’s what I call a patient patient.
9) “Everything is Difficult Until it Becomes Easy”
I have said this phrase thousands of times to patients when starting something new, whether it’s elastics, headgear, or simply just getting accustomed to the braces after the initial bonding. To the kids, I’ll use the analogy of riding a bicycle for the first time: Learning how to steer, balance, and pedal all at the same time is tough. Once they learn how, though, it’s a breeze, and they don’t even think about “how”—they just do it. It’s the same thing with lingual orthodontics. As long as the orthodontist and team recognize this principle and the previous eight tips, then this learning curve can actually be an enjoyable process; and before long, the office will “just be doing it.”
10) Enjoy Specializing Your Practice
Not only does lingual orthodontics offer a unique opportunity for the patient, but it does the same for your practice. Once you have successfully added lingual orthodontics to your practice, you will differentiate your practice from large, managed-care-type clinics; other orthodontists reluctant to advance; and the general/cosmetic dentist using clear aligners or instant orthodontics, veneers, and bonding.
 Recent articles and analyses paint a not-so-rosy picture of our profession’s future based on the last few years. The May 2006 “McGill Advisory” reported results of a 2005 Annual Practice Profitability Survey.3The survey compared production, expenses, and profitability of the seven dental specialties. There were several interesting things that we should note. It revealed that “Orthodontics is the segment of dentistry that has been most adversely affected by the economic changes over the past 6 years (2000–2005). Most orthodontists have seen fewer new patients, and have encountered declining treatment acceptance rates over this time period, leading to fewer case starts. Most practices have maintained stable gross incomes (collections) only due to fee increases, averaging 2–4% annually.”
Recent articles and analyses paint a not-so-rosy picture of our profession’s future based on the last few years. The May 2006 “McGill Advisory” reported results of a 2005 Annual Practice Profitability Survey.3The survey compared production, expenses, and profitability of the seven dental specialties. There were several interesting things that we should note. It revealed that “Orthodontics is the segment of dentistry that has been most adversely affected by the economic changes over the past 6 years (2000–2005). Most orthodontists have seen fewer new patients, and have encountered declining treatment acceptance rates over this time period, leading to fewer case starts. Most practices have maintained stable gross incomes (collections) only due to fee increases, averaging 2–4% annually.”
While some of us may or may not have experienced this trend, the McGill survey had a total of 309 responses, with 65 orthodontic respondents, and it clearly showed how orthodontists’ average gross collections have decreased over the last 6 years, while collections in the other six specialties have increased. If this survey is remotely predictive of our future, we should be concerned.
The survey also reported that, “Combined with increasing treatment efficiency, this decrease in starts has resulted in a dramatic decline in ‘busyness.’ Most orthodontists are now operating at only 70–80% of capacity, the lowest of any segment of dentistry.” In trying to find the cause, it said, “Few orthodontists realize that, in addition to competition from an increased supply of orthodontists, and from general dentists, their biggest competitor is actually producers of other goods and services that are chasing the consumer’s shrinking discretionary dollar.”
Larry White, DDS, MS, wrote a thought-provoking article in the Southern Association of Orthodontists News titled “A Mandate for Change.”4 In it, he drew similar conclusions about how many of our potential patients were being lured by “instant” orthodontics. Many patients, he says, would prefer veneers or cosmetic bonding to enduring “the discomfort of separators, fitting bands, rapid palatal expanders etc and complaining about the seemingly endless number of appointments ….” This is a perception that is driven largely by the media, which reports on the disadvantages of latter-day orthodontic therapy (such as long treatment, discomfort, and inconvenience) and, he says, unfortunately, this is reality in most cases. He argues that our specialty will continue the downhill fall as illustrated by the McGill survey unless we explore new technologies to offer faster, more discreet treatment that is more convenient and less socially intrusive; and, most important, results that not only straighten teeth but also improve facial balance.
Lingual orthodontics, along with other technologies, can give our practices a tool to fill a consumer need that will place us back on top in the world of dentistry. We need to commit to furthering our education. We need to conquer the learning curve. We need to know that our patients are willing to pay for a more aesthetic, less destructive, and more controlled method of giving them the smile, and occlusion, that they want and need. As White concluded, ”We are now better equipped than ever to offer an attractive solution that patients in the new millennium need and will demand. Are you ready? If not, what’s holding you back?”
J. Clifton Alexander, DDS, MS, has practices in Dallas and Coppell, Tex. He is a part-time faculty member in the St Louis University Department of Orthodontics. He can be reached at [email protected].
References
1. Romano R, Decker BC. Lingual Orthodontics. 1998
2. Scuzzo G, Takemoto K. Invisible Orthodontics. 2003, Quintessence Books
3. The McGill Advisory, 21:5, May 2006
4. White L. A mandate for change.Southern Association of OrthodontistsNews. Spring 2006.








