
An orthodontist demonstrates the value of a novel appliance that uniquely comprises the category of “Independent Mover.”
By Isaak Yelizar, DDS
Crossbite malocclusions are usually the result of narrow upper archforms, and present a particular orthodontic challenge, especially as people age. Often, crossbite malocclusions also present with functional shifts. That’s why it’s ideal to intervene early. When we see an adolescent patient with incomplete growth, rapid maxillary expansion is a treatment option—although some parents aren’t particularly open to it.
The fact is, stimulating and addressing dentoalveolar movement, bringing the midlines into alignment, and even achieving Class I occlusion do not always correct the functional shift. Without mandibular shift correction, the adolescent will grow into this deviated chin position, resulting in facial asymmetry, and any pre-existing lack of self-esteem will be heightened. In adulthood, some of these patients will require re-treatment with possible orthognathic surgery to remedy.
Discovering a solution with Brava
A few years ago, I saw a crossbite case Hessam Rahimi, DDS, MSc, MBA, of Dallas, Tex, treated to a beautiful finish with a novel appliance—Brava by Brius Technologies. No expander, crossbite, or midline elastics were used.
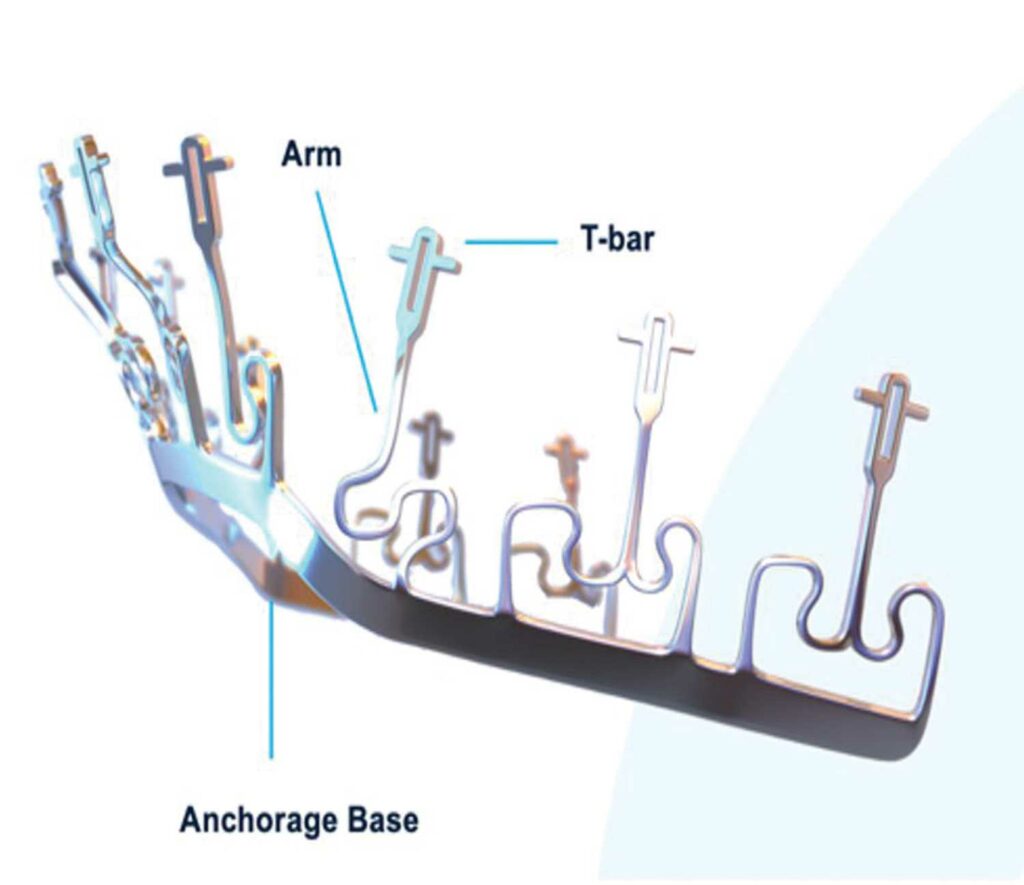
Brava consists of a NiTi anchorage base and pre-programmed NiTi arms that connect independently to each tooth via a customized Brava bracket (Figure 1). According to Brius research, the anchorage base absorbs much of the reactive forces that occur in any continuous archform, rendering them clinically insignificant. This Independent Movement puts Brava into its own category of orthodontic systems. The force and movement programmed into Brava’s NiTi arms put each tooth on an independent path to its planned destination. Brava eliminates wire sequencing, complex aligner mechanics and sequences, and compliance.
When a case similar to that of Rahimi presented in my practice, I called him to discuss Brava and became enthusiastic to employ it with my patient.
Case review: history and diagnosis
A female patient, age 11 years, 2 months, presented at her initial consultation with a severe functional shift of her mandible. Even without completing her intraoral exam, I knew I would be dealing with a transverse discrepancy.








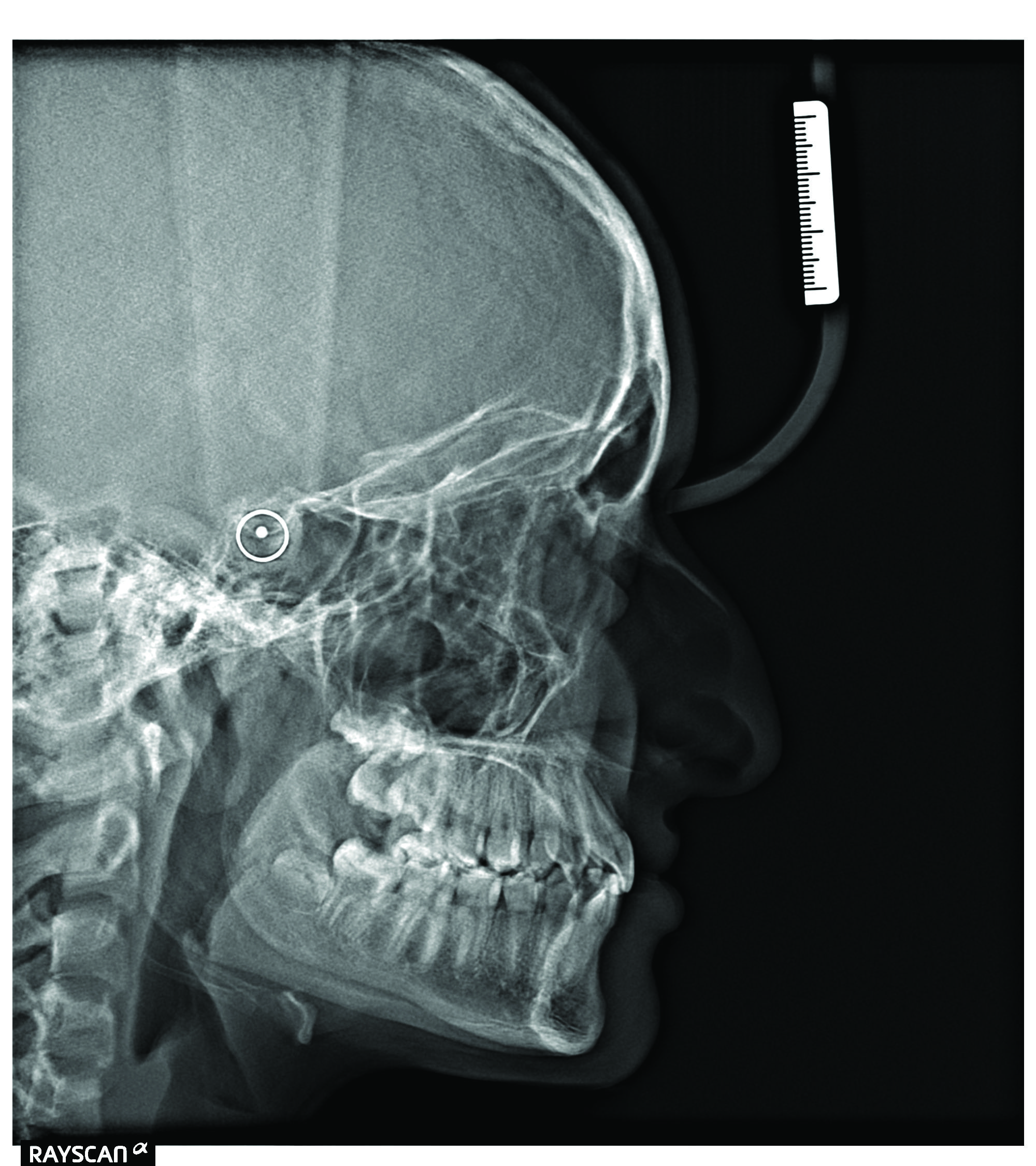

Figure 2. Initial records: Crossbite with 6 mm upper arch transverse deficiency.
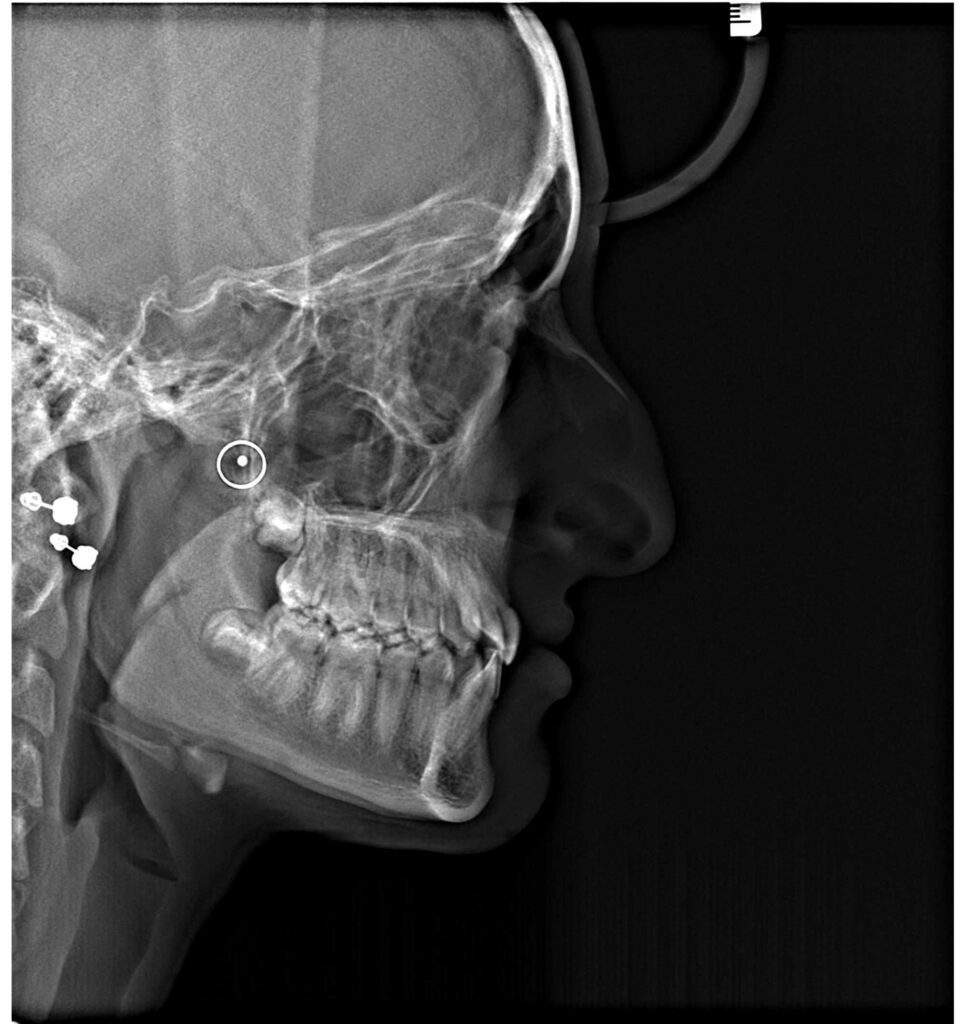
The transverse deficiency of her upper arch, 6 mm at the molars, with a restricted triangular shape, had caused her lower jaw to shift to the right (Figure 2). The mandibular arch was a normal parabolic U-shape. The panoramic X-ray showed the 7s still erupting and the 8s developing, which I recommended be assessed by an oral surgeon in her mid-teens. The cephalometric X-ray demonstrated a brachycephalic facial pattern with a strong gonial angle.
Treatment recommendation and plan
After a thorough examination, I knew the treatment plan would be simple: expand the upper arch and eliminate the transverse discrepancy to achieve facial symmetry. Because of the patient’s young age, surgery wasn’t recommended; however, due to her maturation stage, I was a bit concerned that the window for skeletal expansion was closing fast. The majority of the crossbite correction would be dentoalveolar in nature with either the use of a traditional expander or Brava.
When provided both options, the patient and parents agreed on Brava. A 3D scan was taken the same day and was submitted to Brius Technologies. My patient was excited to have an aesthetic means to a beautiful smile, especially without any expanders, or cross elastics, etc.
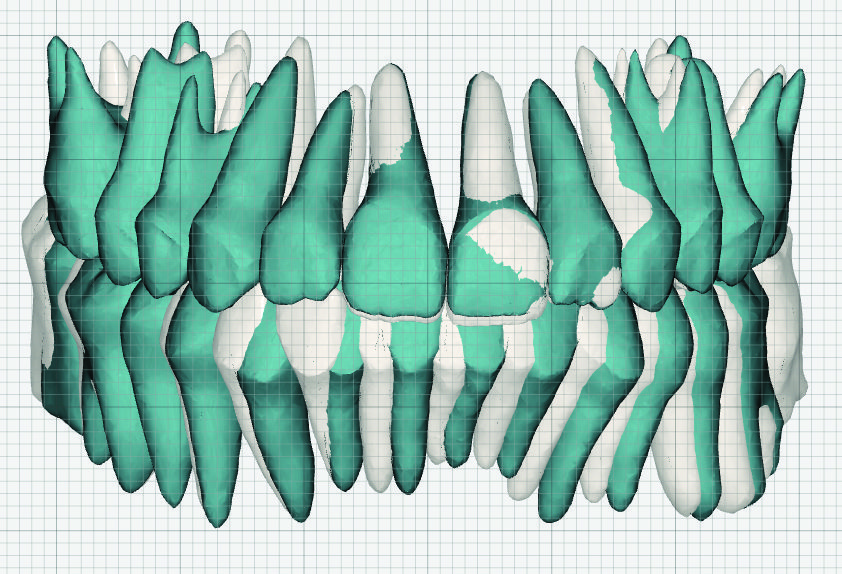


Figure 3: Brava treatment plan in Brius’s interactive software. The white teeth are the initial tooth positions; the blue overlay, the setup.
The treatment plan (Figure 3) was to maintain the lower archform and develop and coordinate the upper arch, eliminating the functional shift. I found that Brius Technologies advanced 3D software controls make treatment planning visually appealing as well as easy to use. Controlled dentoalveolar movement of the upper right posterior quadrant was planned to expand the upper arch.
Brius Planner Software is highly interactive. Starting with the proposed Brius setup, I was able to move each tooth to the desired, final position without the need to communicate movements to technicians through notes, as is required with many other customized orthodontic software.


Figure 4: Bonding: Upper arch with disarticulation. Bonding both arches, same day is now my protocol.
Bonding with disarticulation with Brava
Once I approve a setup, Brius Technologies fabricates and ships Brava, usually within 2 weeks. After receiving the appliance for this patient, we bonded the upper arch (6-6). Resin disarticulators were placed on the U6s (Figure 4) to aid in eliminating premature contacts and to expand the upper arch gradually with the very low NiTi forces. The lower arch was bonded 7-7 2 weeks later. Today, all my Brava patients have both arches bonded same day within 90 minutes.
What’s interesting with crossbite cases are Brava’s NiTi arms which sit close to the center of resistance of each tooth, effectively achieving expansion through translation rather than tipping. I’ve found that no conventional appliance can mimic Brava’s arch development mechanics in terms of speed and efficiency. I was actually amazed at the amount of controlled expansion achieved in only 2 weeks, in a brachycephalic patient with strong masseter muscles.
A word about bite blocks. I consider disarticulation essential to eliminate functional shifts in crossbite cases. While disarticulation is not a recommended Brava protocol, I use it quite often but usually with minimal buildup.


Figure 5: Two weeks: Midline is halfway corrected with only Brava and bite turbos. Note the arch form development.


Figure 6: Two months: Midlines are aligned and arch form is parabolic. Again, without any wire changes, elastics, or other intervention.
In 2 weeks, and with only the use of Brava and bite turbos, the mandible had shifted slightly to the left and the midline had already halfway corrected. The upper arch was also developing nicely (Figure 5). At 2 months, without the use of elastics or wire changes, the lower arch had shifted, and the facial asymmetry had improved. In comparing via photos her initial mandibular chin position to the 2-month mark post-bonding, we were able to appreciate how much facial change had occurred. From this point on, it was just a matter of controlling the bite to correct the occlusion. The upper arch form was now nicely coordinated and I knew then that the case would finish beautifully (compare Figures 4 through 6.) To be able to provide such facial correction without surgery is the greatest gift orthodontists can provide to their patients. It’s performing plastic surgery without a scalpel.

Figure 7: Six months: First Brava NiTi refinement to address Class III growth tendency.

Figure 8: Ten months: Second Brava NiTi refinement to pick up the 7s.
At 6 months, the NiTi arms of the original Brava had fully expressed themselves, and since the patient had a Class III jaw growth tendency in need of control, the first Brava NiTi refinement scan was taken (Figure 7) with the second one taken at 10 months to pick up the 7s (Figure 8). We scan for refinements with the brackets in place so the Brius Planner Software can utilize current bracket positions.
In most cases, after approximately 6 months, when the Brava NiTi arms have expressed their forces, Brava can remain in place to continue elastics wear, if needed. A scan can be taken for a Brava NiTi refiner or a Brava finishing refiner. I know of no other bracket-and-wire appliance that provides this type of refinement system.
Note: If a bracket debonds, we rebond the bracket by segmenting the Brava digital bonding tray (DBT) and tucking back the Brava arm. Once rebonded, we engage the Brava arm. What would be a 40-minute appointment with other appliances, I find takes mere minutes with Brava.
Midway through treatment, ceramic buttons were bonded for elastics (3.5 oz, 3/16″) to control for Class II and Class III force vectors and to achieve a Class I socked-in occlusion. Be sure to advise patients that while Brava’s independent movement offers advanced, pre-programmed biomechanics, natural but unaccounted for variables can result in minor tipping or spacing that either self-correct or are easily corrected with Brava refiners by the end of treatment.

Figure 9: Fifteen months: Custom Brava refiners delivered. Note the smile width.
At 15 and 17 months, custom Brava refiners (Brius aligners provided at no extra cost) were delivered for fine-tuning. Any brackets and labial buttons are left in place to serve as attachments, with button cutouts. Note how broad and beautiful her smile is in Figure 9.









Posttreatment discussion
Even with time required for the second molars to erupt, the case finished in 19 months. There were 10 visual visits and six active visits (Figures 10 and 11). Since this was an early Brava case for me, and I was interested in closely tracking her progress, her appointment intervals were set at 4 weeks. Eight weeks is now standard in my practice.

The patient and her parents were happy and excited about the result. We achieved all our dental and facial goals with a 12-tooth smile and the effect of plastic surgery without surgery. By diagnosing and planning the case correctly, treatment was executed using only Brava, resin bite turbos, and some light interarch elastics. The result is a beautiful arch shape and width, good interarch coordination and tooth alignment with midlines on, appropriate overbite and overjet, and a socked-in Class I occlusion. With the crossbite corrected and the mandibular shift eliminated, I feel the case demonstrates the simplicity and effectiveness of Brava.
Conclusion
The beauty of this Brava treatment is that we’ve changed this patient’s life without extractions, patient-dependent heavy elastics, a functional expander, or surgical intervention. I certainly could not have accomplished such a gratifying result with aligners alone. After just 2 months, we were already seeing the beginning of facial balance change and with treatment completed, she will continue to grow into a beautiful young woman, full of life and confidence. It’s miraculous how much we can positively affect a person’s life by changing facial esthetics with orthodontics alone.
Since this case, I have further used Brava in my practice. I can recommend it not only for complex cases such as the one presented here, but for routine cases as well. I would not want doctors to think Brava should be reserved for complex cases alone. Brava’s Independent Mover technology has significant treatment advantages that I noticed immediately. Having such a straightforward, capable treatment option that can resolve cases in as much as half the time with less energy than other options has been a real boon for my practice and I am grateful to have discovered such a powerful tool that will continue to be an important part of my armamentarium. OP

Isaak Yelizar, DDS, is a board-certified orthodontist in private practice in Queens, NY. He received his doctoral degree in dental medicine from the New York University College of Dentistry, earning the highest honors and several scholastic awards. He furthered his clinical skills in general and restorative dentistry at New York Methodist hospital, before completing his orthodontic training at St. Barnabas Hospital in the Bronx, NY. Yelizar has considerable experience in a wide range of treatment modalities, giving particular consideration to achieving facial balance, and has a keen interest in incorporating new and transformative technologies into his practice.








