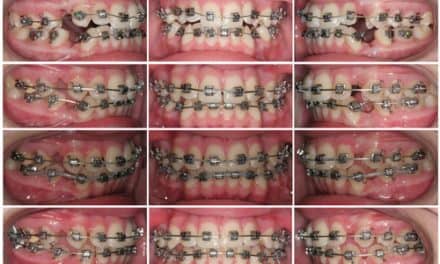
Figure 1: Initial
Anterior open bite malocclusions are universally considered to be challenging cases. They are traditionally treated surgically with a Le Fort I maxillary impaction. Surgery comes with many risks and inconveniences. Surgery is also very expensive and in some instances cost prohibitive, oftentimes causing patients to be reluctant or completely resistant to orthognathic surgery.
Non-surgical orthodontic correction of anterior open bite malocclusion is commonly achieved by dental extrusion through the use of either inter-maxillary elastics or a combination of extractions and elastic wear. This type of treatment has proven to be inherently unstable, frequently resulting in relapse of the anterior open bite.
An alternative non-surgical approach to anterior open bite correction is posterior dental intrusion using skeletal anchorage. This treatment approach has been more favorable with regard to relapse. It also has allowed for “skeletal change” through autorotation of the mandible. The ability to change the mandibular plane angle, lower facial height and chin projection is very useful in the correction of Class II malocclusions which frequently accompany anterior open bite.
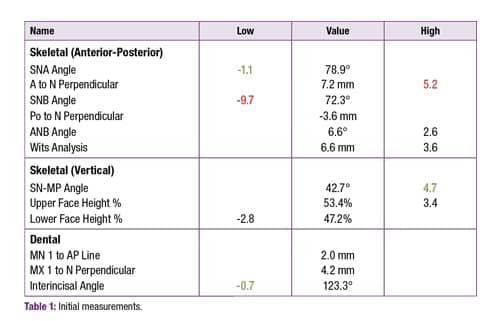
Table 1: Initial measurements
Diagnosis
A 32-year-old female presents for her third orthodontic opinion. The patient has a history of orthodontic treatment as an adolescent and reports changes in her bite and the appearance of her smile since the completion of previous treatment, consistent with relapse. She presents with both a skeletal and dental Class II relationship, a narrow maxilla relative to the mandible resulting in a unilateral posterior cross-bite, and an anterior open bite. Both previous orthodontists’ treatment plans consisted of comprehensive fixed orthodontics in conjunction with orthognathic surgery involving a two piece Le Fort I maxillary impaction to correct the open bite and narrow maxilla and a mandibular bilateral sagittal split osteotomy for the A-P correction. The patient was adamantly opposed to surgery.
Treatment Plan
Comprehensive non-extraction orthodontic treatment with 3M Unitek’s Clarity™ ADVANCED Ceramic Brackets with APC™ Flash-Free Adhesive and TAD assisted intrusion of the posterior dentition to facilitate Class II and anterior open bite correction through mandibular autorotation.

Figure 2: Three month progress; day of TAD placement.

Figure 3: Eight month progress.
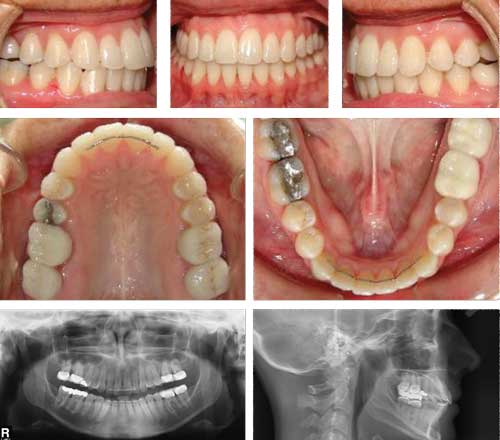
Figure 4: Final—at 12 months.

Table 2: Final measurements.
Discussion
Treatment duration was 1 year. Class II inter-maxillary elastics were not used to correct the Class II discrepancy and vertical elastics were not used to close the anterior open bite. Inter-maxillary elastics were used during finishing stage to help settle and detail the occlusion. Changes in cephalometric measurements between the initial and final time points in a non-growing patient help to illustrate what occurred solely as a result of treatment. Class II skeletal indicators: ANB was reduced from 6.6 degrees to 4.2 degrees. The Wits analysis was reduced from 6.6 mm to -1.7 mm. Vertical skeletal indicators: MP-SN was reduced from 42.7 degrees to 36.7 degrees. The occlusal plane steepened from 22 degrees to 26 degrees, indicating intrusion of the posterior dentition and resultant mandibular autorotation. Of course, there will be some compromises without orthognathic surgery. The primary compromise in this case was the transverse discrepancy and resultant torque discrepancies in the posterior dentition.
In conclusion, posterior dental intrusion using skeletal anchorage is a useful tool for stable, predictable, non-surgical correction of anterior open bite malocclusion. OP
 Cranford Shane Langley, DMD, MS, received his DMD from the University of Alabama School of Dentistry and an MS and Orthodontic Specialty Certificate from the University of Alabama at Birmingham. He has been in private practice since 2009, and is currently an adjunct assistant professor in the Department of Orthodontics at the University of Alabama. He is a member of the American Dental Association, American Association of Orthodontists, Alabama Dental Association, Baldwin County Dental Study Club, and Mobile Area Dental Society.
Cranford Shane Langley, DMD, MS, received his DMD from the University of Alabama School of Dentistry and an MS and Orthodontic Specialty Certificate from the University of Alabama at Birmingham. He has been in private practice since 2009, and is currently an adjunct assistant professor in the Department of Orthodontics at the University of Alabama. He is a member of the American Dental Association, American Association of Orthodontists, Alabama Dental Association, Baldwin County Dental Study Club, and Mobile Area Dental Society.