
by Ron Roncone, DDS, MS
How to make the most of your day, 5 minutes at a time
 |
No practice can function efficiently and with little stress if it does not schedule properly. This is why scheduling is listed first among my “17 Critical Factors for the Orthodontic Practice.” This article will address several problems that have slowly crept into the philosophy of scheduling.
There is no such thing as an average day.
By this I mean a day when a practice can see four new patients, 2½ starts, three removals, 22 arch changes, six retention checks, etc. That day does not exist except in the imagination of consultants. I would defy any practice to show me more than a handful of days during a year that would fit such a schedule. The appointment coordinator has to “fudge” many times during the day.
 |
| Ron Roncone, DDS, MS |
We do not schedule patients!
We schedule staff members to do specific procedures or jobs at specific times. For example, each registered dental assistant is scheduled to be at a specific chair or chairs and will see 20 to 30 patients per day within specific time allotments for each procedure. Each treatment coordinator (we call them patient consultants) is scheduled to see three to six new patients per day along with the orthodontist at a specific time of the day. Time is allocated for the new patient tour, database intake, the clinical examination, a PowerPoint presentation, financial arrangements, printing appropriate letters to give to the patient that day and send to the general dentist and physician, and setting up an appointment for diagnostic records and initial bonding. The financial coordinator posts payments and makes deposits at a specific time of the day. An insurance coordinator handles all insurance during specific times of the week or month and will not be interrupted by other duties. I think you are beginning to get the point.
The clinical team is much more efficient when they are performing “like things at like times.”
This idea was proposed by Jay Barnett, DDS, many years ago. Our practice has carried this philosophy to a logical extreme by scheduling bondings at the same time and no other types of appointments at that time. Arch changes, retainer checks, and removals are all scheduled in the same manner. A very important aspect of this philosophy is that we schedule all new-patient consultations in succession. As an example: New patients are scheduled from 8 am to 10 am and 2 pm to 3 pm every 20 minutes (of doctor time). Using the same example, that would mean six new patients in the morning and three new patients in the afternoon. We use two or three PCs occupying different rooms to accomplish this. No other patients are scheduled during this time. Assistants and other staff members are doing their other necessary ancillary jobs at this time instead of trying to get them done “in between” patients.
Each month is not the same!
Therefore, schedules should change based on past practice history. Most, if not all, orthodontic practices are busier in July and August than they are in February and December. Other months may be “average.” Therefore, we might increase the number of new-patient consultations in our busiest months and decrease them in slow months. Why stress over trying to fill these slots in a historically slow month? It also creates wasted time that could be scheduled for procedures that are needed, such as arch changes. Setting up a schedule for a year should be logical.
Every day does not have to be the same.
With the advent of self-ligation, we have eliminated a large number of wire changes and a whole classification of appointment: re-ties. This allows us to see bondings not only in the mornings but also in the afternoons if we so choose.
Rules for scheduling:
- Determine your average patient interval (6, 8, or 10 weeks). To do this:
- Identify the last 25 patients who have finished full, comprehensive treatment.
- Count the number of appointments they had while they were in treatment, from initial placement to debonding. (This includes any emergency appointments they may have had.)
- Determine the number of weeks they were in treatment.
- Divide the number of weeks into the number of appointments.
- The appointment interval is the average number of weeks between appointments.
- Count every appointment that was scheduled during that interval.
- Time all procedures that are performed in the clinic. Time each assistant doing each procedure three times. By doing this three times, you can get the average for each assistant. When timing procedures, you must count checkout, instructions, and cleanup time as part of the procedure.
- Decide which of the collective times are acceptable for you to build your schedule around.
- Color-coordinate appointments by procedure and doctor-time, with “like” things at like times.
- Do not fill every available slot. The patient will just be waiting in the chair because the doctor will not be available anyway.
Do not schedule an “average” or “typical” day after you have gathered all this information. You need only to provide enough time in each patient cycle for the various types of procedures that will be needed. For example, if you see patients every 8 weeks, and on average you need 60 hours of arch change or adjustment time during that period, you can allot that time in any way you prefer, then divide it by the number of chairside assistants.
For example, if you had four chairside assistants, you would divide the 60 hours by four; and therefore, each assistant would be responsible for 15 hours of arch-change time in an 8-week period. Please understand that the number of hours needed is only an example and does not necessarily reflect what is the true requirement for a practice. Use this system for each type of procedure until your schedule is completed.
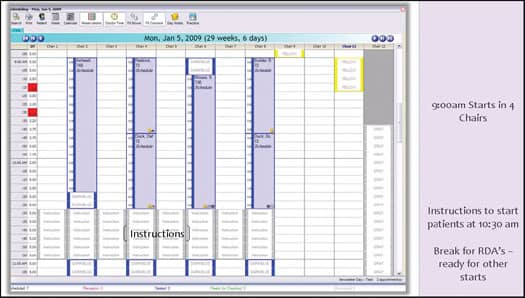 |
| Figure 1: Every day’s schedule is unique. |
And remember, each month is not the same. Therefore, the schedule should be different. The schedule shown as an example (Figure 1) may be great for January, March, April, May, and October, but you might need fewer new-patient consultation slots in February, June, September and November, and more slots in July and August.
You should use 5-minute scheduling increments. No total procedure from check-in to checkout can be accomplished in 5 minutes. However, this increment gives the most flexibility. If you use a 10-minute increment and the full time required for the appointment is 15 minutes, there will be 5 minutes of “wasted” time. If you are on 15-minute intervals and a procedure takes 20 or 25 minutes, you are wasting 5 to 10 minutes of time.
In the sample schedule, no two days are exactly the same. For example, one day per week is devoted to debonding and TMD patients in the morning. The afternoon is scheduled for retainer inserts of the morning’s debond patients and retention check/adjustment appointments.
For our patient’s convenience, we schedule three different types of days in terms of start and end times:
- 6:30 am to 3 pm
- 7 am to 4 pm
- 8 am to 4:30 pm
Another essential factor in scheduling is to remember that some patients fall outside the typical times provided for a specific procedure. If a procedure normally would take 10-5-20—that is, 10 minutes of assistant time followed by 5 minutes of doctor time, and 5 minutes of “checkout” time for a total of 20 minutes—it may be perfect for a teenage boy. But it is not the correct time for an adult who needs to ask questions. This adult is happy asking questions of the chairside assistant; therefore, the appropriate time would be 15-5-25. Five additional minutes is added for the assistant at the next appointment. Neither of these times are appropriate for the patient who must speak to the orthodontist. Therefore, an appropriate time for the exact same procedure might be 10-10-25 or even 10-15-30. This can be determined at the chair and added “on the fly” as necessary.
|
To see a list of companies that offer scheduling software, check out our Buyer’s Guide. |
Our system of doctor-time scheduling allows greater flexibility for your patients and a less stressful day for your assistants—and it creates greater efficiency. Whether you are looking to create more revenue by seeing more patients or to decrease your workload by working fewer days, our scheduling system is designed to give you the power to be in control of your schedule.
Ron Roncone, DDS, MS, is in private practice in Vista, Calif. He has presented more than 600 seminars around the world and is president and CEO of Roncone Orthodontics International®. He can be reached at








