by Neal D. Kravitz, DMD, MS
Regaining control of invisible tooth movement
 |
| Neal D. Kravitz, DMD, MS |
Anterior lingual braces, placed canine-to-canine, offer a noncompliant, aesthetic alternative to removable orthodontic aligners. While the origin of lingual braces dates back more than 30 years, they have had a low level of popularity outside of Europe, Asia, and Australia. Recently, lingual orthodontics has undergone a resurgence among American professionals and manufacturers looking to address the limitations of orthodontic aligners. This article will provide a brief overview of two anterior lingual systems, Ormco’s STb Social 6TM and GAC’s Innovation®-LMTM, and compare their advantages to those of removable aligners.
Historical Perspective
Lingual braces began in the 1970s when two independently working orthodontists—the late Craven Kurz, DDS, of Beverly Hills, Calif, and Professor Kinja Fujita of Kanagawa Dental University in Japan—developed their own systems for placing braces on the inside surfaces of teeth.1 Interestingly, in Japan, the development of a lingual appliance was not a result of an aesthetic demand as in the United States, but was rather to protect the lips and cheeks of patients who participated in martial arts.2 The first lingual prototypes were simply modified labial braces.1 In 1976, Kurz submitted the first lingual appliance patent to the US Patent Office, and 3 years later, with the collaborative work of Craig Andreiko, DDS, MS, and Ormco Corp, the popular Ormco-Kurz lingual bracket system (1979) was fabricated.1,2
 |
| Figure 1: An STb Social 6 bracket. |
In the 1980s, lingual orthodontics developed slowly in North America as orthodontists struggled with the lingual technique, which required different treatment planning and a different approach to biomechanics, as well as challenges with ergonomics and treatment efficacy. With the concomitant development of “tooth-colored” labial brackets made from single-crystal sapphire and later from ceramics, the early excitement of lingual orthodontic treatment dimmed, and much of the advancement of lingual orthodontics occurred outside the United States. Since 2000, with the boom of Invisalign®, removable orthodontic aligners rather than lingual braces have become the treatment alternative for patients seeking invisible orthodontics.
Lingual orthodontics is undergoing a process of simplification due to advancements in indirect bonding and bracket design.3 In particular, there has been a recent growing interest in lingual braces limited to the anterior teeth as an easy-to-learn, noncompliant, invisible alternative to removable orthodontic aligners.
Reason for the Lingual Resurgence
 |
| Figure 2: An In-Ovation-LMTM bracket. |
The recent resurgence in lingual orthodontics is likely attributed to clinicians seeking a more economical, effective, and efficient treatment alternative to removable aligners. The most notable limitations of aligners are the high laboratory costs, the dependency on patient compliance, and the limitations in tooth movements.
Clinical studies have shown the least predictable tooth movements with removable aligners are incisor extrusion, canine/premolar rotation, and root uprighting.4,5 Additionally, such tooth movements often require bulky tooth attachments (to increase the tooth’s geometric mass and enhance undercuts within the aligner), which many patients find unsightly. Therefore, even a simple Class I malocclusion that requires extrusion of the maxillary lateral incisors or derotation of the mandibular canines may not be suitable for removable orthodontic aligner treatment.
STb Social 6 and In-Ovation-LMTM
Clinicians experienced with removable aligners know that the predicted treatment results are often not achieved clinically, either due to limitations in the aligner material or poor patient compliance. Final detailing often requires costly refinement or a brief period of traditional labial orthodontics, which is often frustrating for both the patient and the clinician. In search of a more cost-effective and efficient treatment for addressing the “social six” anterior teeth, many clinicians have turned to segmental anterior lingual orthodontics, such as the STb Social 6 and the In-Ovation-LMTM.
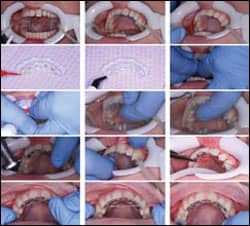 |
| Figure 3: IDB bonding of STb Social 6. First line: isolation, etching, and application of Ortho Solo. Second line: placement of Ortho Solo on bracket pad, placement of composite on bracket pad, insertion of the transfer tray. Third line: curing of the transfer tray with lingual pressure, removal of the hard outer tray, removal of the soft inner tray. Fourth line: removal of flash, cleaning interproximally with serrated strips, wire insertion (straight-length 0.013 NiTi). Fifth line: space consolidation with energy chain on 0.017 x 0.017 TMA. |
The STb was developed for Ormco by two of the leading lingual practitioners in the world—Giuseppe Scuzzo, MD, DDS, (third president of the European Society or Lingual Orthodontics, ESLO) and Kyoto Takemoto, DDS—as the first lingual straightwire bracket and technique. The STb (Scuzzo/Takemoto bracket) is a full-arch lingual bracket system. It has a low 1.5-mm profile and rounded contours to reduce lingual interference and minimize speech difficulties. In addition to its small size, its design is a significant advancement in the field of lingual orthodontics, because it facilitates the use of light forces and low friction.2,6
The STb Social 6 (Figure 1, page 41) is an anterior lingual bracket, indirectly bonded either canine-to-canine or first premolar-to-first premolar, designed for correcting minor-to-moderate anterior crowding or spacing with maximum control. Often, no more than two wires are needed to unravel the teeth, without the need for finishing bends.
The In-Ovation-L was developed in 2007 by Ron Roncone, DDS, MS, and GAC International as a lingual bracket utilizing the patented Passive-Interactive-Active self-ligating clip of the popular In-Ovation-R bracket. The In-Ovation-L, like STb, is a full-arch lingual system. In 2008, with the collaborative efforts of Roncone, the In-Ovation-LMTM (Minor Tooth Movement) anterior lingual bracket was developed for addressing minor misalignments canine-to-canine. The In-Ovation-LMTM maintains the passive-active self-ligating clip of the progenitor bracket, with a smaller pad size for easier placement and improved patient comfort (Figure 2, page 41).
Clinical Indications
The STb Social 6 and the In-Ovation-LMTM systems are appropriate for the following conditions:
- Crowding of 6 mm or less;
- spacing of 3 mm or less;
- midline correction of 2 mm or less; and
- rotations of 25º or less.
Getting Started
You can order STb Social 6 brackets through AOA Laboratory. AOA also will provide the indirect bonding setup and transfer tray for its lingual brackets. In-Ovation-LMTM brackets are directly bonded to the patient. Currently, no laboratory provides indirect bonding for the In-Ovation-LMTM.
-
For the STb Social 6, take upper and lower polyvinyl siloxane impressions with a bite registration. Fill out the STb Social 6 prescription form, which is available online at www.aoalab.com/index/AOAlab-Education. You can even request the laboratory to return chairside adhesive with the transfer tray.
Check “STb Social 6” in the first box of the prescription form, and complete any special instructions as needed. If you are derotating canines or consolidating space distal to the canine, request the addition of first premolar brackets.
The indirect setup provided by AOA Laboratory is a double tray using a clear 0.30-inch hard outer tray and a translucent polyvinylsiloxane inner tray to allow for light curing. All STb Social 6 and most STb cases do not require full Torque Angulation Reference Guide (TARG) or Custom Lingual Appliance Setup Service (CLASS) setups for indirect bonding. This simplifies the indirect bonding setup and reduces the laboratory cost.
Typically, if the brackets are bonded to the lingual surfaces without a setup, the archform must be customized to the shape of the patient’s dentition.7 However, the combination of the straightwire STb system with AOA Laboratory’s indirect bonding allows for prefabricated nickel-titanium, TMA, or stainless-steel wires.
-
Bond or indirect bond the brackets. After bonding, thoroughly clean interproximally and at the palatal or lingual gingival margin, where flash often accumulates. I recommend using 0.006-inch interproximal strips with a serrated edge to saw between contacts (Figure 3).
If you are bonding the upper anterior teeth, check for lower incisor contact against the brackets; if contact is heavy, consider occlusal buildups on the posterior teeth (Figure 4). You may consider using blue-colored occlusal buildup material (I use Ultra Band-lok from Reliance Orthodontic Products). This stops the patient from thinking that his or her tooth has fractured if the buildup comes off during treatment.
-
For crowded cases, begin with the straight-length 0.013-inch CuNiTi wire for the STb Social 6 or the straight-length 0.12-inch Sentalloy for the In-Ovation-LMTM, which come included with purchase of the brackets. For spacing cases, consider starting with 0.016-inch lingual NiTi. You may consider using a traditional (labial) lower-arch NiTi extending canine to canine. The only disadvantage of using a labial wire rather than a mushroom-shaped lingual wire is that the canines may expand and roll out distally if left unmonitored.
-
Following tooth leveling and alignment, a 0.016-inch stainless-steel or 0.017 x 0.017-inch TMA wire can be placed for finishing bends and space closure. The STb Social 6 brackets are ligated with standard alastic ties, while In-Ovation-LMTM uses a self-ligating clip. Due to the short interbracket distance, I recommend closed Energy Chain® (Rocky Mountain Orthodontics) for space consolidation.
-
Treatment duration with either of these systems is approximately 3 to 9 months, often requiring only one or two wires. At the completion of treatment, the brackets are easily debonded with a pin and ligature cutter.
 |
| Figure 4: Occlusal buildups can prevent contact of lower incisal edges. |
 |
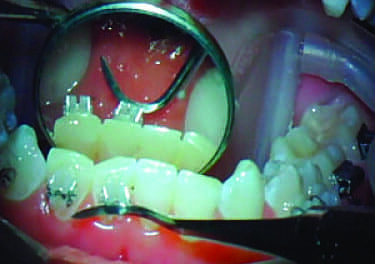
| Figure 5: Intraoral photos of a patient currently in treatment in upper and lower STb Social 6. Note the invisibility of the brackets and proper rotational correction of the canines. The lower right central incisor still needs more alignment prior to debonding. |
Anterior Lingual Braces Versus Removable Aligners
Anterior lingual brackets offer the following advantages over removable aligners:
- Anterior lingual braces do not require patient compliance other than following dietary and hygiene instructions.
- All tooth movements, including translation, rotations, and extrusions, are highly predictable.
- Lingual braces are 100% invisible, unlike aligners, which can become cloudy or require the use of bulky attachments. (Figure 5).
- The low profile of the STb system allows for proper intercuspation during alignment, unlike aligners, which often result in a posterior open bite at the commencement of treatment.
- The laboratory expense is approximately $200, which is one-fifth the cost of aligners.
- Anterior lingual systems often require fewer appointments and shorter treatment time.
In short, the STb Social 6 and In-Ovation-LMTM systems offer a simplified lingual solution for addressing aesthetic concerns without compromising treatment results.
Neal D. Kravitz, DMD, MS, is in private practice in White Plains, Md, and South Riding, Va. He is a diplomate of the American Board of Orthodontics, and is on the faculty at the University of Maryland and Washington Hospital Center. He can be reached at
References
- Ling PH. Lingual orthodontics: history, misconceptions and clarification. J Can Dent Assoc. 2005;71:99-102.
- Echarri P. Revisiting the history of lingual orthodontics: a basis for the future. Semin Orthod. 2006;12:153-159.
- Mujagic M, Fauquet C, Calletti C, Palot C, Wiechmann D, Mah J. Digital design and manufacturing of the Lingualcare bracket system. J Clin Orthod. 2005; 39: 375-82.
- Nguyen CV, Chen J. In: Tuncay OC ed. The Invisalign System. New Malden, UK: Quintessence Publishing Co Ltd; 2006: 121-132.
- Kravitz ND, Kusnoto B, Agran B, Vianna G. Influence of attachments and interproximal reduction on the accuracy of canine rotation with Invisalign. Angle Orthod. 2008: 87:682–687.
- Scuzzo G, Takemoto K. Invisible Orthodontics. Current Concepts and Solutions in Lingual Orthodontics. Berlin, Quintessenz Verlags-Gmbh, 2003.
- Macchi A, Tagliabue A, Levrini L, Tressi G. Philippe self-ligating lingual brackets. J Clin Orthod. 2002;36:42-45.