
How one practice uses Propel and AcceleDent to accelerate the biology of tooth movement
By David Alpan, DDS, MSD
When are my braces or treatment going to be completed?” I get this question multiple times each day. Eventually, I started to turn this question back around on my patients, asking them, “When will their treatment be finished?” They always look at me funny and say, “You’re the doctor. You tell me.” My typical response is, “In a few visits.”
We, as orthodontists, have a reputation of extending treatment due to our desire to create perfection. The problem we are dealing with is a wide variety of malocclusions, ethnicities, teeth sizes, bone biologies, and various levels of compliance. It is not an easy question to answer, and many times the answer is really an estimation based on our clinical experience. Unfortunately, none of us can predict treatment time with 100% accuracy, but we all are trying to incorporate as many technologies as possible to become more efficient. And now, accelerating the biology of tooth movement is one more modality to add to our armamentarium.6,18,19,20,21
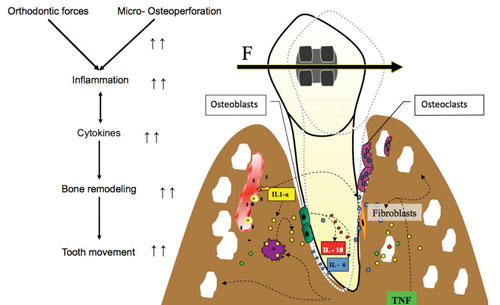
Figure 1: The biology of tooth movement with micro-osteoperforations (MOPs).
The practice of orthodontics is about the science of the biology of tooth movement17 (Figure 1). My study of this science began as a senior dental student, with my research project on the influence of secondary messengers on calcium regulation in osteoblasts. My mentor, Kenneth Snowdowne, PhD, and I were interested in finding the secondary messengers for calcium regulation so we could influence osteoblasts and osteoclasts calcium regulation. We were attempting to understand how to accelerate the biology of tooth movement. This project was awarded first place from the ADA/DENTSPLY Student Research Competition in 1995, at the University of the Pacific Dental School, and I was invited to present my research at the Student Clinicians of the American Dental Association (SCADA) at the 37th annual ADA convention in Las Vegas that year.
We sought to determine which mechanism of increased calcium in the cell could regulate cyclic nucleotides in the arachidonic acid cascade. Our research found that the arachidonic acid cascade has no effect on cyclic nucleotides. Overall, stretch of the cell was still the main stimulator to increase calcium intracellular.22 Our goal throughout was to isolate a messenger such as cytokines or create a drug that could attach to the proper receptor so we could influence the biology or rate of tooth movement.
When I graduated from my orthodontic program in 1998, the concepts of accelerated orthodontics revolved around mechanical efficiency. Trauma, sound, light, and vibration were all being studied, but nothing was definitive. There is a long history in orthodontics looking at the various mechanical appliances and their efficiency in tooth movement, including prescription brackets, straight wire mechanics, self-ligating versus non self-ligating, clear brackets with various levels of friction, passive versus active self-ligation, biomechanics with loops via Burrstone mechanics, constant non-decaying force applications such as nickel titanium wires, and nickel titanium springs. We found lighter constant forces were easier for the biology to adapt, with less pain and root resorption.

Figure 2: Large molar spaces
In the early 2000s, the old concept of high forces and more regular visits were still popular, but I found myself moving into lighter forces and fewer visits. As an early adopter of the Ormco’s Damon passive self-ligation (PSL), I saw the benefits of frictionless movement. The improved mechanical advantage reduced treatment time, leading me to believe we had accelerated tooth movement. Most of my cases finished ?6 months faster with Damon PSL, but detailing was more challenging. Leveling and aligning became super easy, but the AP and transverse corrections still took time to correct.

Figure 3: Molar spaces closed in 8 months with Damon TADs and use of Propel.
Ten years later, after more research in the field of accelerated orthodontics, various products and techniques began to emerge. Now, in my practice, with the use of Damon PSL braces, a TAD, and two to three treatments with the Propel device or with consistent patient use of AcceleDent® 20 minutes daily, closing a first molar space is possible with minimal side effects (Figures 2; Figure 3). Reduction in treatment time is now directly controlled by choosing more efficient appliances in conjunction with accelerating the biology of tooth movement.

Figure 4: Performing MOPs with Propel.
The biology of tooth movement research showed that if inhibiting the expression of certain cytokines decreases the rate of tooth movement,7 then creating an iatrogenic trauma to stimulate the expression of inflammatory cytokines through small micro-osteoperforations (MOPs) (Figures 4 and 5) of the cortical bone, we would find that the rate of bone remodeling would increase and ultimately, so would the rate of tooth movement.1

Figure 5: Propel light is activated at a designated depth.
The idea of traumatizing the bone is not new and is now correlated with the increase in the inflammatory cytokines that can increase bone remodeling (Figure 1).6 In fact, previous studies had demonstrated that bone injury, which causes cytokine release, leads to accelerated bone turnover and a decrease in regional bone density.2,3,4,5,8

Figure 6: Large diastema
Since the public launch of AcceleDent by OrthoAccel Technologies Inc in early 2012 and Propel by Propel Orthodontics in late 2012, clinicians are seeing incredible results with accelerating the biology of tooth movement. I find that the clinical research states a 50% to 60% increase in tooth movement,6 but this does not correlate to the same reduction in overall treatment time. In my practice, we are seeing on average a 40% reduction in overall treatment time, independent of the appliance choice in my practice. We currently use Propel or AcceleDent in conjunction with Invisalign, Incognito, and Insignia/Damon. We are finding that MOPs can be used on all types of difficult cases such as severe crowding or spacing (Figures 6 and 7), all of our TAD cases, impacted teeth,19 intrusion of gummy smiles,19 extraction cases, or molar protraction.21 My favorite application is for any difficult or stubborn tooth. Our biggest success with Propel has been with existing patients that need to get completed in less time or have already gone over their estimated treatment time and are anxious to get finished. Some of our extended treatment cases have resolved themselves with the help of one or two Propel treatments.

Figure 7: Space closed in 4 months
The Propel technique is clearly outlined and explained by Nicozisis,18 who outlines the benefits as decreased treatment time, which minimizes side effects and avoids the complications of long-term orthodontic treatment. In my practice, we are finding a reduction in decalcification, white lesions, root resorption and/or blunting, and overall patient satisfaction with decreased treatment time when using either Propel or AcceleDent. After all, the faster we complete treatment, the happier the patient will be. And the decrease in the number of visits leads to more profitability for the practice, independent of how the practice charges or does not charge for using these devices.21
Treatment Protocols
When treating, I place two to three holes interdentally usually vertically aligned from the crest, and I
usually start with a 3 mm hole and then 5 mm, and then 7 mm if possible. Propel has three depth settings and an automatic light indicator is triggered at the desired depth (Figure 5). The last hole tends to be in the mucosal tissue, while the first hole is always in attached tissue.
Little to no pain is experienced by the patient postoperatively—usually 1 to 2 days of mild discomfort in the local area.6,18,20,21 Some patients require the use of a local anesthetic via syringe, but in most cases, topical gels and Madajet are sufficient. We start with benzocaine 20% for 3 to 5 minutes locally, then a compounded topical (Lido 10% Prilocaine 10% and Tetracaine 4%) for 30 to 60 seconds, followed by a Madajet with Lidocaine 2% 1:100,000 epi spray. This is the same technique used for my TAD placements.
When I began to introduce accelerated orthodontics with Propel and AcceleDent, I found that there was a need to change our appointment intervals, seeing patients sooner. Patients who choose AcceleDent need to be compliant 20 minutes daily. We check the compliance interface at each visit, giving us a chronologic history by day, month, time, and length of use. With Propel there is no issue of patient compliance, as MOPs are performed every 6 to 12 weeks depending on the need. When using Propel reactively, patients typically require one to two sessions of MOPs, but patients who want to reduce total treatment time proactively from the initial appointment may need three or more sessions.
With our Invisalign patients we change aligners every 7 to 10 days, and we give them one to start and then three to four at each visit. If treatment is progressing nicely, we may graduate to delivering six aligners at each visit. We typically plan for one refinement as part of the finish. For our Incognito patients we are seeing them every 4 weeks for wire activations or changes. Insignia/Damon patients are seen every 4 weeks for wire changes. Our non-Insignia/Damon cases come in every 4 weeks to assist us in our repositioning of brackets or finishing techniques.
Practice-Management Protocols
The cost of these systems will, of course, be a factor for the patient. And they do differ, with AcceleDent costing more for both me and the patient compared to the Propel device. With the Propel device’s lower cost, I choose not to charge some patients, as the benefit of completing treatment is greater. The advantage of AcceleDent, however, is that it requires no doctor chairtime and is less clinical work if the patient is compliant. And when the cost of either device is compared to the alternative of Wilkodontics™, where the typical surgical price ranges from $5,000 to $10,000 and carries with it the risk of side effects, the cost of either device can be minimal.
Orthodontic fee agreements are usually spread out over the length of the treatment time, especially as patients appreciate the convenience of paying for the treatment over time. Since our accelerated orthodontics has changed our original estimated treatment time, it has been necessary to change existing patients’ contracts. We have had some challenges with our new patients, since we don’t have as much time to amortize their treatment fee. For some patients, we have extended the payment arrangements past the finish date. However, we ask most patients to complete payment by the end of treatment.
Conclusion
I have found my introduction with accelerated orthodontics to be very rewarding for me and my patients. It is now part of my everyday practice. I discuss the benefits of AcceleDent and Propel with all my patients. The benefits of decreased treatment time far outweigh any of the costs or additional work. Using AcceleDent in conjunction with any orthodontic appliance will decrease sensitivity and reduce treatment time. Performing MOPs with the use of Propel has clinically shown to increase the rate of tooth movement. Completing treatment early, with fewer visits and decreased side effects, are compelling reasons to introduce accelerated orthodontics into your daily practice. OP
 David Alpan, DDS, MSD, received a DDS degree from UOP and was licensed in California and Nevada in 1996. He earned an Orthodontic Specialty Certificate in 1998 and was awarded a MSD for his research on TMJ. Alpan founded his private practices, Alpan Orthodontics, in Los Angeles, Beverly Hills, and Las Vegas in 1999. He played an integral role in Align Technologies Clinical Education Department, serving as a consultant and speaker for 6 years. He is a member of Ormco Insiders and a part of 3M Unitek’s research panel.
David Alpan, DDS, MSD, received a DDS degree from UOP and was licensed in California and Nevada in 1996. He earned an Orthodontic Specialty Certificate in 1998 and was awarded a MSD for his research on TMJ. Alpan founded his private practices, Alpan Orthodontics, in Los Angeles, Beverly Hills, and Las Vegas in 1999. He played an integral role in Align Technologies Clinical Education Department, serving as a consultant and speaker for 6 years. He is a member of Ormco Insiders and a part of 3M Unitek’s research panel.
References
1. Teixeira CC, Khoo E, Tran J, Chartres I, Liu Y, Thant LM, et al. (2010) Cytokine expression and accelerated tooth movement. J Dent Res. 2010;89:1135-1141.
2. Frost HM. The regional acceleratory phenomenon: a review. Henry Ford Hosp Med J. 1983;31:3-9.
3. Frost HM. The biology of fracture healing. An overview for clinicians. Part I. Clin Orthop Relat Res. 1989;248:283-293.
4. Frost HM. The biology of fracture healing. An overview for clinicians. Part II. Clin Orthop Relat Res. 1989;248:294-309.
5. Shih MS, Norrdin RW. Regional acceleration of remodeling during healing of bone defects in beagles of various ages. Bone. 1985;6:377-379.
6. Alikhani M, Raptis M, Zoldan B, et al. Effect of the micro-osteoperforations on the rate of tooth movement. Am J Orthod Dentofacial Orthop. 2013;144(5):639-48.
7. Arias OR, Marquez-Orozco MC. Aspirin, acetaminophen, and ibuprofen: their effects on orthodontic tooth movement. Am J Orthod Dentofacial Orthop. 2006;130:364-370.
8. Yaffe A, Fine N, Binderman I. Regional accelerated phenomenon in the mandible following mucoperiosteal flap surgery. J Periodontol. 1994;65:79-83.
9. Adachi Y, Okazaki M, Ohno N, Yadomae T. Enhancement of cytokine production by macrophages stimulated with (1–>3)-beta-D-glucan, grifolan (GRN), isolated from Grifola frondosa. Biol Pharm Bull. 1994;17:1554-1560.
10. Alhashimi N, Frithiof L, Brudvik P, Bakhiet M. Orthodontic movement Arend WP, Palmer G, Gabay C. IL-1, IL-18, and IL-33 families of cytokines. Immunol Rev. 2000;223:20-38.
11. Arias OR, Marquez-Orozco MC. Aspirin, acetaminophen, and ibuprofen: their effects on orthodontic tooth movement. Am J Orthod Dentofacial Orthop. 2006;130:364-370.
12. Basaran G, Ozer T, Kaya FA, Hamamci O. Interleukins 2, 6, and 8 levels in human gingival sulcus during orthodontic treatment. Am J Orthod Dentofacial Orthop. 2006;130:E1-6.
13. Dale DC, Boxer L, Liles WC. The phagocytes: neutrophils and monocytes. Blood. 2008;112:935-945.
14. Davidovitch Z, Nicolay OF, Ngan PW, Shanfeld JL. Neurotransmitters, induces high numbers of cells expressing IFN-gamma at mRNA and protein levels. J Interferon Cytokine Res. 1988;20:7-12.
15. Dienz O, Rincon M (2009). The effects of IL-6 on CD4 T cell responses. Clin Immunol. 2009;130:27-33.
16. Henneman S, Von den Hoff JW, Maltha JC. Mechanobiology of tooth movement. Eur J Orthod. 2008;30:299-306.
17. Krishnan V, Davidovitch Z. On a path to unfolding the biological mechanisms of orthodontic tooth movement. J Dent Res. 2009;88:597-608.
18. Nicozisis JL. Accelerated orthodontics through micro-osteoperforation. Orthodontic Practice. 2013;4(3):56-57.
19. Guinn. Propel orthodontics enabling faster and more predictable results. Orthotown. 2013;38-41.
20. Pobanz, Storino, Nicozisis. Orthodontic acceleration: Propel alveolar micro-osteoperforation. Orthotown. 2013;1-4
21. Nicozisis. Accelerated tooth movement technology. Orthotown. 2013;1-4.
22. Garlet TP, Coelho U, Silva JS, Garlet GP. Cytokine expression pattern in compression and tension sides of the periodontal ligament during orthodontic tooth movement in humans. Eur J Oral Sci. 2007;115(5):355-362.







