
by Mark R. Yanosky, DMD, MS
Managing treatment and enhancing aesthetics
Orthodontic patients are interested in more than just “straight teeth.” They are interested in well-aligned, beautiful white teeth; ideal function and occlusion; ideal gingival aesthetics; well-proportioned faces; and gorgeous smiles. Furthermore, patients would like for this to be accomplished in a reasonable amount of time. Recently, the soft-tissue laser has gained attentionas an effective tool to help manage treatment and enhance our aesthetic outcomes. The soft-tissue laser can significantly reduce treatment time by creating access for brackets/bands, improving bracket placement by improving tooth proportionality, and helping manage oral hygiene through removal of pseudopockets. Gingival aesthetics can be enhanced through shaping and contouring the gingival tissue during treatment, at appliance removal, and even in retention. Other articles1–3 have described laser technology, the potential uses of soft-tissue lasers in clinical orthodontic practice, and the technique for performing the procedure. This article will review uses of diode soft-tissue lasers in the orthodontic office, and discuss how lasers can be an effective tool for your practice.
Creating Access for Bracket Placement
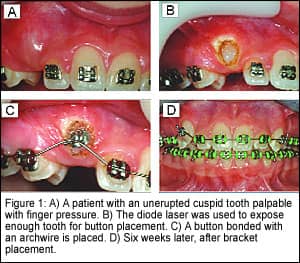
With the tremendous pressure we are under to finish treatment in a timely manner, it is frustrating to wait for completion of passive eruption for treatment to proceed. The diode laser can be used to remove tissue (gingivectomy and gingivoplasty) and provide access for bracket/band/button attachment. These procedures provide earlier attachment to teeth and can significantly reduce treatment times. Commonly, cuspids are some of the last teeth bonded due to slow eruption, delayed passive eruption, or impaction. This becomes a treatment-management issue when treatment time runs longer than estimated; it is a functional issue if the cuspids cannot be bracketed ideally, resulting in lack of cuspid guidance and coupling; and it can be a stability issue if extruded cuspids are debonded prior to allowing these teeth to stabilize. Archwire bends are required if the bracket cannot be placed ideally, resulting in increased chairtime and difficulty in finishing treatment. The posterior occlusion is often hindered by delayed passive eruption of the second premolars. As it does with the cuspids, this results in archwire bending, increased chairtime, and increased treatment time to finish the case. Operculums on second molars often prevent banding of these teeth, resulting in increased treatment time to await further eruption. The diode laser can be used to assist the clinician in avoiding these situations by going directly to attachment, bracket, or band placement (Figure 1).
 Establishing Tooth Proportionality
Establishing Tooth Proportionality
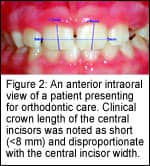
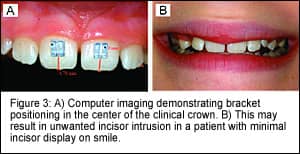
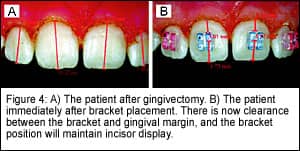
Most clinicians position brackets (directly or indirectly) either by measuring a prescribed distance from the incisal edge or visualizing and positioning the bracket in the center of the clinical crown. Both methods are acceptable and have performed adequately for many years. Problems with these bracket-positioning methods tend to arise when the clinical crown is not equal to the anatomic crown in length, a common finding in adolescent orthodontic patients (Figure 2, page 20). Measurement from the incisal edge may result in an acceptable occlusal outcome, but may result in poor oral hygiene due to encroachment of the bracket on the gingival margin. Bracket position in the center of the clinical crown would be too incisal, resulting in unwanted incisor intrusion and reduction of incisal display at rest and on smile (Figure 3). The diode laser can be used at the initial placement visit, prior to positioning, to improve proportionality and allow the position of the central incisors to be maintained in the smile (Figure 4).
|
Oral Hygiene
Adolescent patients often have a difficult time with oral hygiene. Most offices will go over oral-hygiene techniques with their patients, recommend a fluoride rinse, and ask patients to keep their oral-hygiene recall visits with their general practitioner. When these basic methods are not getting the job done, archwire removal and referral to the general practitioner, increased frequency of cleaning appointments, and even appliance removal is occasionally needed. Chronic poor oral hygiene in orthodontic patients results in gingival overgrowth, pseudopocket formation, and plaque-retention problems—not to mention increased treatment times, unhappy patients and parents, and ultimately a less-than-desirable cosmetic result. We can hope that improved oral hygiene would result in improved tissue, but the reality is that a poor brusher during treatment is often a poor brusher after treatment. These problems are difficult to overcome by the patient alone, and are rarely resolved completely using the traditional methods.

The diode laser can be used to remove the pseudopockets, providing access for patients to improve their oral hygiene and providing better access for topical fluoride application. This procedure can often be combined with gingival contouring for improved gingival aesthetics, and can be performed at any point during treatment or at the debonding visit itself (Figure 5, page 22).
Apthous Ulcer Management
Patients will often present for an appointment and say, “Please be careful; I have an ulcer in my mouth.” Various rinses and topical anesthetics can be offered to the patient, but this appointment is at best uncomfortable for the patient. Sometimes, the entire appointment needs to be rescheduled, resulting in a negative experience and increased treatment time. The diode laser can be used in noncontact mode (1 to 2 mm away from the tissue) to irradiate the ulcer for approximately 30 seconds. In our experience, the patient reports an immediate reduction of pain. The procedure creates a nonpainful laser wound that replaces the painful ulceration. The patient is generally able to tolerate the appointment much easier at this point.
Gingival Contouring and Shaping
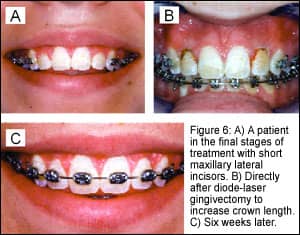
Gingival shape refers to the 2D curvature of the gingival margin. Gingival-shape problems include gingival margin discrepancies and improper zenith (apex of the curvature of the gingival-margin for a given tooth) locations. Gingival contour refers to the 3D architecture of the gingiva characterized by sharp interdental papillae and tapered gingival margins. Gingival-contour problems include rolled margins and inflamed papillae. Adolescent orthodontic patients will very often have short clinical crowns due to incomplete passive eruption or asymmetric crown heights and rolled margins due to marginal oral hygiene. These problems become noticeable in the finishing stages of treatment and can be exacerbated by poor oral hygiene. Crown lengthening via gingivectomy can serve to enhance the aesthetic outcome by improving tooth-to-tooth proportionality and arch symmetry (Figure 6, page 22). While we prefer to perform these procedures midtreatment (when resetting brackets for final detailing) rather than at the debonding appointment so that final tooth adjustments can be made if necessary, we frequently will shape and contour the gingiva at the debonding appointment or during retention.
Debonding Day
The day on which appliances are removed should be a positive experience for the clinician, patient, and parent. Nothing is more disheartening than debonding a challenging orthodontic case where an ideal occlusal result was obtained, only to have a disappointed patient or parent due to inflamed, puffy gingiva. These gingival-shape and contour problems create a visual distraction. The soft-tissue laser allows you to improve the result immediately by shaping and contouring the gingival tissue to a more desirable position.
A Word of Caution
The soft-tissue laser is not a cure-all. Several factors need to be evaluated in patients prior to performing a laser procedure. First, the patient’s smile needs to be evaluated prior to aesthetic procedures to see if the gingival margin is even visible. If not, the laser procedure may be contraindicated. Second, it is essential to measure for adequate biologic width. In areas of minimal attached gingiva (less than 1 mm), the laser may be contraindicated and an apically positioned flap may be required. Bone level and tooth wear need to be evaluated in cases of asymmetric crown heights, as intrusion and restoration may be more appropriate than gingivectomy. The patient may also desire more crown lengthening than is possible with soft-tissue laser gingivectomy due to bone levels. In all of the above cases, a periodontal referral is indicated.
Incorporating the Soft-Tissue Laser Into Everyday Practice
A common concern of orthodontists who are considering using a soft-tissue laser in their clinical practice is, “Will my referral sources, other specialists (especially periodontists), and my patients accept the use of the laser in my office?” The most appropriate way to approach this is to discuss the issue with your referral sources and specialists. When explained from the standpoint of treatment management, oral-hygiene control, and reduced treatment time, it usually makes sense to the referring doctor. We further explain that we do not charge an additional fee for the laser procedures but consider it an added service. Most doctors appreciate that.
From the aesthetic standpoint, we consider the shaping and contour-ing procedures a “touch-up” similar to the reshaping of uneven incisal edges. We do not make any effort to pass ourselves off as periodontal specialists. One key to incorporating the soft-tissue laser into your practice is understanding the indications and contraindications, and always communicating with your referring doctor regarding these instances. Our patients have been very accepting of the soft-tissue laser. Due to the small size, the fact that it requires topical anesthetic only, and the minimal doctor time involved, we have been able to incorporate the laser into our everyday schedule easily. We have even had parents of patients request that we use the laser on their child.
In summary, the soft-tissue laser can be an effective tool in your practice to reduce treatment times, control oral hygiene, and enhance the final result of your cases. If used properly, it can increase practice efficiency and be a practice builder for you in your community.
Mark R. Yanosky, DMD, MS, is in private practice in Vestavia Hills, Ala. He can be reached at [email protected].
References
1. Hilgers JJ, Tracey SG. Clinical uses of diode lasers in orthodontics. J Clin Orthod. 2004;38(5):266–273.
2. Sarver DM, Yanosky M. Principles of cosmetic dentistry in orthodontics: Part 2. Soft tissue laser technology and cosmetic gingival contouring. Am J Orthod Dentofacial Orthop. 2005;127(1):85–90.
3. Sarver DM, Yanosky M. Principles of cosmetic dentistry in orthodontics: Part 3. Laser treatments for tooth eruption and soft tissue problems. Am J Orthod Dentofacial Orthop. 2005;127(2):262–264.







