by Gerald Nelson, DDS
A systematic approach to decreasing treatment time with a full fixed appliance
Treatment efficiency is an elusive goal and one every clinician desires, since it can dramatically affect the bottom line and reduce the risk of damage to hard and soft tissues. A very efficient protocol is to conduct comprehensive treatment in 22 visits, including the records visit, start appointments, all adjustments, the debanding visit, and two retention visits. Every appointment that is added beyond this goal will reduce the per-visit income and will subject the patient’s oral tissues to extended challenge. One cannot expect to meet this goal with every patient, but it forms a framework in which to gauge your on-time status. You could strive for achieving a goal of 22 visits in 75% of cases.
Work Versus Adjustment Visits
Efficiency has much to do with standardization, attention to doctor time, and putting similar procedures together. When a patient arrives for a bonding or banding procedure, for example, equipment setup is more complicated and the procedures performed by the assistant and orthodontist are more extensive than those for an adjustment appointment. This is true whether three attachments are placed or a full fixed appliance is placed. If you are to treat a patient in 22 visits, it is wise to minimize work appointments, thereby conserving doctor time. Placing a full fixed appliance in stages is not an efficient use of resources, nor is doing bracket resets at several points during treatment. Sometimes, treatment procedures preliminary to full fixed appliances are necessary. For example, it is usually best to delay placement of the full appliance in canine-impaction cases, because management of the canine will interfere with the normal pace of treatment (Figure 1).
 |
| Figure 1: Retrieving a canine preliminary to comprehensive treatment. |
Once the canine is in the arch, you can proceed with full fixed appliances. In 22 visits, the ideal number is three work visits (appliance placement, corrective resets, and appliance removal); all other visits should be adjustments, and they can probably be scheduled in the after-school hours. Other procedures that might be done in a preliminary stage are maxillary expansion, lower lingual arch, bite planes or bite turbos, functional appliances, or headgears.
Appointment Interval
Practice consultants have urged orthodontists to have longer intervals between patient visits. This makes sense only if the tooth movement is progressing during the entire interval. When NiTi wires are used, the force application is fairly steady over a long range of tooth movement, which supports the idea of longer appointment intervals. When steel wires are used for detailing adjustments, the range of movement is approximately 1 mm, so a long appointment interval can extend treatment time (Figure 2, below). While this does not degrade the clinician’s efficiency, it enhances risks of root-end resorption and soft-tissue disease.
 |
| Figure 2: NiTi wire stays in the optimum range much longer. |
Given these considerations, my recommendation is to schedule 6- to 8-week intervals for wire systems that will move teeth less than 1 mm and 3- to 4-week intervals for movements greater than 1 mm.
Organizing Treatment Into Three Phases
Orthodontic treatment with full fixed appliances can be sectioned into three distinct phases, which promote better efficiency, delegation of assistant duties, and control of outcome quality. Each of these phases has criteria that will affect the archwires you choose and the sequence you employ. In some cases, the period of full fixed appliances may be preceded by a period of preparatory work such as retrieving an impacted tooth or rapid maxillary expansion. I will describe each phase and the rationale for archwire choices and sequence.
Alignment Phase
The alignment phase involves placing the appliance, correcting bracket positions using an x-ray to evaluate root positions (Figure 3), aligning the teeth, beginning archform changes such as expansion, and beginning extraoral traction. It should take 6 to 8 months and include four to five visits at 6- to 8-week intervals. Most efficient is to place the full appliance at the beginning, including second molar attachments. Second choice would be to delay placing the second molar attachments until the next work visit, when bracket positions are evaluated and corrected.
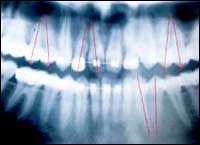 |
| Figure 3: Evaluate root positions in the alignment phase. |
The corrective reset visit is done during the second archwire, usually before the sixth month of treatment. To plan the corrective reset visit, you will make a careful visual assessment of bracket positions, noting marginal ridge discrepancies, irregular incisor levels, or uncorrected rotations, and a radiologic assessment, noting root displacements. Noted discrepancies are all corrected at the same visit, along with placement of second molar attachments if they are not already in place. The archwires used should provide a light, continuous force with a 3- to 4-mm interbracket range; the cross-sectional size should almost fill the bracket, and the archwire surface should offer minimal friction with the bracket slot. The wire should not be deformable by normal mastication. The alignment phase is the appropriate time to begin cross elastics or extraoral traction. Space closing or Class II or III elastics should not be done on NiTi wires, to avoid excess tipping of teeth or the occlusal plane.
These criteria demand a NiTi wire. There are a number of choices, and below are specific recommendations.
- Slot size 0.018 ligature-tie bracket: The first wire could be in the stiffness range of an 0.012 NiTi. This will provide rapid alignment even with 3- to 4-mm displacements (Figure 4, below right). The next wire (6 to 8 weeks later) could be a square, superelastic wire that nearly fills the slot, such as the 0.0175 x 0.0175 heat-activated (HA) wire with a 6° torque loss (3M Unitek). While this wire is in place, evaluate all bracket positions using both visual and radiographic assessment. This evaluation will usually lead to resetting two to five brackets. If second molars were not placed, this is the time to do it.
- Slot size 0.022 ligature-tie bracket: If you use the 0.022 bracket, you will use larger wires for the alignment phase. At the University of California, San Francisco (UCSF), we recommend starting with 0.014 NiTi and proceeding to a 0.020 x 0.020 HA wire with 7° torque loss to finish the alignment phase.
- Slot size 0.018 ligation-free bracket: Since there is no ligature to push the archwire to the base of the bracket, a square cross-section wire is not the best choice. A rectangular wire will improve rotational control, so after beginning with an 0.014 NiTi, switch at the second visit to the 0.016 x 0.025 HA (9° torque loss) to finish the alignment-phase procedures, including resets.
- Slot size 0.022 ligation-free bracket: Again, a larger size is appropriate, with a goal of keeping force values low. Start with the 0.014 NiTi and proceed to 0.018 x 0.25 HA (15° torque loss).
Once the full appliance is in place, corrective resets are done, and the teeth are aligned, you can proceed to the working phase.
Working Phase
 |
| Figure 4: A 3-mm displacement with 175 x 175 HA. |
During the working phase, which can last 6 to 12 months and include four to eight visits at 6- to 8-week intervals, arches are coordinated, all spaces are closed, molars and cuspids are put in proper digitations, midlines are aligned, overbite and overjet are corrected, occlusal planes are flattened, and occlusal tables are corrected. Corrective resets done in the alignment phase should ensure level marginal ridges, symmetrical incisal-edge relationships, lined-up central grooves, and proper rotations of individual teeth.
To achieve these goals, the archwire should engage the bracket slots with slot play that is cancelled by the bracket prescription. For example, retraction of incisors where slot play is 8° would demand an incisor preadjustment of 15° torque to result in the ideal 7° torque at finish. The wire should offer low friction and not be easily deformed by mastication, but be adjustable by the clinician, including forming closing or intrusion loops. This last criterion takes NiTi wires off the list. The force levels should allow a 1-mm vertical adjustment in-between brackets. Should you use square or rectangular wires? This question is less relevant than asking what is the slot play. A square wire that compares with a rectangular wire in slot play will give you lower forces for the same adjustment. If you prefer lower forces or want a larger range to your adjustments, the square wire is more logical.
The archwire must deliver enough force to alter archform, level occlusal planes (even against parafunction), bodily retract incisors, and prevent teeth from tipping into extraction space during space closure. Here are some archwire recommendations for the working phase.
- Slot size 0.018 ligature-tie bracket: For closing spaces, use the 0.0175 x 0.0175 SS archwire (6° torque loss) with closing loops bent into the arch. Alternatively, use the same archwire with closing modules such as AlastiK chain or NiTi closed-coil springs. This wire has the power to alter archform, flatten the occlusal plane, and bodily retract incisors.
- Slot size 0.022 ligature-tie bracket: UCSF residents use 0.019 x 0.025 SS wires (11° torque loss) for space closing with loops or retraction springs. Sometimes, torque adjustments are placed in the upper anteriors to ensure bodily movement.
- Slot size 0.018 ligation-free bracket: Use 0.016 x 0.025 SS, close space with closing loops or with closing spring modules.
- Slot size 0.022 ligation-free bracket: Use 0.019 x 0.025 SS as with the ligature-tie brackets.
Once all spaces are closed, arches are coordinated, and overjet and overbite are close to correction, you can then move to the finishing phase.
Finishing Phase
During the finishing phase, which should last 6 to 8 months and include five to eight visits, the clinician will finalize arch coordination, including midline synchronization and canine function. Small vertical detail adjustments or archwire bends to correct very minor rotations will provide good centric stops and interdigitation. The patient may still be on intermaxillary elastics or headgear to hold corrections. Although major torque discrepancies should have been corrected in the working phase, good torque control (especially of molars and incisors) is essential to an optimum outcome, which means slot play must be accounted for in the bracket prescription.
The archwire should have enough stiffness to hold corrections in archform and occlusal plane, and to resist damage from mastication. The wire should allow a 1-mm vertical interbracket adjustment and 25° of torque without distressing the patient. The clinician may want a wire that allows soldering of hooks. This precludes the use of NiTi wires for these finishing functions.
Wire recommendations for the finishing phase are the following:
- Slot size 0.018 ligature-tie bracket: 0.0175 x 0.0175 SS (6° torque loss).
- Slot size 0.022 ligature-tie bracket: 0.019 x 0.025 SS (11° torque loss).
- Slot size 0.018 ligation-free bracket: 0.016 x 0.025 SS (9° torque loss).
- Slot size 0.022 ligation-free bracket: 0.016 x 0.022 SS (11° torque loss).
The archwires described above can be used to develop a very simple archwire sequence that will handle all challenges in typical comprehensive orthodontic treatment. The sequence is fairly simple. Using the 0.018 slot ligature-tie appliance, it would be:
- 0.014 NiTi
- 0.0175 x 0.0175 HA
- 0.0175 x 0.0175 SS
Using the 0.018 slot ligature-free bracket:
- 0.014 NiTi
- 0.016 x 0.025 HA
- 0.016 x 0.025 SS
 |
| To implement these ideas, browse for “brackets” in our online Buyer’s Guide. |
This supports the notion that if the archwire choices are based on the goals of each phase of treatment, then the force application is coordinated with the desired range of movement.
Conclusion
Appliance and biomechanical strategies should be standardized. Organizing the fixed-appliance treatment process can profoundly affect efficiency. Three distinct phases of comprehensive fixed-appliance therapy based on the principles discussed here will enable efficient treatment within 22 visits while facilitating an excellent outcome. Defining the functions of the three phases will lead to logical archwire choices based on bracket prescription, slot play, stiffness, force delivery, and desired range of movement.
Gerald Nelson, DDS, is the UCSF Orthodontic Division Vice Chair, and has been in private practice in Berkeley, Calif, for 35 years. He is a diplomate of the ABO, Editor-in-Chief for the Pacific Coast Society of Orthodontists Bulletin, and a delegate to the AAO House of Delegates. He can be reached at








