
by Marcel Korn, DMD
How to resolve crowding by using flexible lip bumpers in the middle mixed dentition
Introduction
The resolution of crowding has taken many directions, ranging from arch widening to arch development, extraction of dental units, and functional development.
This article will make the case for the “middle mixed dentition” as the optimal timing for the resolution of crowding with a “redirection of eruption” approach.
 Our treatment method will be initiated when all the Cs, Ds, and Es are still present, and 50% of the root of the permanent first bicuspid has developed.
Our treatment method will be initiated when all the Cs, Ds, and Es are still present, and 50% of the root of the permanent first bicuspid has developed.
History and Rationale
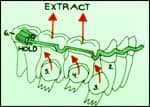
In an effort to develop an early-treatment regimen that obviates a nonextraction approach, we developed a system of maxillary and mandibular lip bumpers in conjunction with a bite plane. The primary objective was to change the direction of eruption of permanent cuspids and bicuspids, and thus allow for unraveling of the erupting permanent teeth. Because permanent cuspids are displaced mesially and labially in dental-crowding situations, it is considered desirable to create a path of lesser resistance and allow the permanent cuspids and bicuspids to erupt more distally and buccally.
The roots of the primary molars are seen as obstacles to a redirection of the path of eruption. Thus, early extraction of the primary teeth should remove these obstacles and allow permanent cuspids and bicuspids to erupt in a less-crowded environment.
Panoramic films taken at appropriate times during development help determine the optimal time for primary tooth removal. Primary tooth removal should not be considered until succedaneous permanent root development (one half root) is such that primary tooth extraction would not lead to damage or retarded eruption. Panoramic films should be taken periodically to evaluate adequate permanent root maturity.
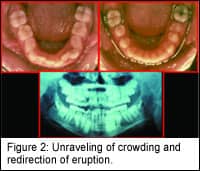
The results of this approach are quite dramatic: marked unraveling, relief from crowding, and bite opening.
Eruption Patterns, Molar Rotation, Crowding, and Overbite
Our current preliminary research indicates that the variables of crowding, overbite, and maxillary molar rotation are prevalent (82%–95%) in a majority of the conditions encountered in orthodontic practice. In addition, when crowding is noted in the mixed dentition, preliminary research indicates that developing permanent tooth buds are angulated, rotated, or partially ectopic at a statistically significant rate.
The issues of crowding, overbite, and maxillary molar rotation must be priorities of the first phase of treatment. If not, then they must be addressed in the second phase or fixed-appliance phase, thus lengthening both the second phase and the total treatment time.
This helps explain why some early-treatment research has shown Phase I and Phase II treatment to be inefficient, more lengthy, and more costly. Such research outcomes have thus been negatively influenced by appliance design, prioritization of objectives, and failure to address crowding, molar rotation, and ectopic eruption prior to permanent tooth eruption.

|
Redirection of Eruption Our research indicates that 75% of crowding cases exhibit radiographic findings consistent with angulation, rotation, or partial ectopia of developing permanent tooth buds, and/or uneven resorption of primary tooth roots. These factors illuminate the necessity for redirecting the paths of eruption of permanent tooth buds, and thus make a strong argument for the middle mixed dentition as an optimal time to start treatment. Treatment Method Our therapeutic method prioritizes the management of crowding, overbite, and molar rotation during the first phase of treatment. The treatment method incorporates disocclusion, redirection of eruption, maxillary molar rotation, and transverse and vertical control. Our therapeutic method employs a new family of modular, fixed-removable appliances that combine the benefits of the European functional concepts with the control of American fixed appliances. Flexible maxillary and mandibular lip bumpers are used in combination with a bite plane and sequential primary tooth extraction to create an environment that allows the tongue to be the formative force during enhanced permanent tooth eruption. Disocclusion is accomplished with the bite plane. Space maintenance is achieved with the lip bumpers. Redirection of eruption is accomplished with the properly timed sequential extraction of primary teeth. Maxillary molar rotation is achieved with the maxillary lip bumper. Transverse controls come with the lip-bumper effect. Vertical control is managed with the bite plane. Arch Development Mechanical widening of the arches has largely been replaced in orthodontics by the use of such procedures as sutural opening, functional appliances that limit the constricting effect of the buccal musculature, and transpalatal arches that rotate, upright, and expand the maxillary molars. This article presents a technique that optimizes nonextraction treatment by incorporating flexible lip bumpers, bite planes, and selective extraction of primary teeth to correct crowding, deep overbite, and narrow archform. As with Frankel’s buccal shields, the maxillary and mandibular flexible lip bumpers minimize restrictive cheek and lip pressures and allow arch development and relief of crowding, while promoting molar distalization and controlling molar rotations. Lip bumpers simulate the effects of Frankel’s vestibular labial pads, while achieving greater patient cooperation than with Frankel appliances or headgear. Our appliance uses flexible wires for even greater patient comfort. Bite planes are added to remove occlusal restrictions, permitting tooth movement and eruption, while a combination of maxillary and mandibular lip bumpers remove both muscular and occlusal restrictions that impede lateral and vertical development. |

Effects of the Lip Bumpers
The maxillary lip bumper
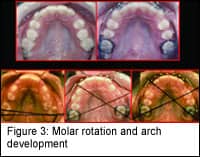
1) rotates the maxillary molars distally with a headgear effect produced by lip pressure transmitted to the molars. This action is reinforced with lip-seal exercises;
2) removes lateral and labial restrictions on eruption, per- mitting lateral dentoalveolar development;
3) rotates the maxillary molars through the activation of termi- nal bends at the molar tubes; and
4) maintains palatal expansion by minimizing the constrictive pressure of the buccal musculature.
The mandibular lip bumper
1) maintains space in the arch;
2) controls and corrects molar rotations; and
3) permits lateral dentoalveolar development by limiting the pressure of the buccal musculature.
Design and Placement of Lip Bumpers
The lip bumpers are made of malleable, .040-inch stainless-steel wire with preformed vertical loops and posterior adjustment bends. The vertical loops maximize lip contact in the maxilla and allow anteroposterior adjustments in both arches.
Fitting and insertion of the bumpers simply requires the placement of molar bayonet bends that act as posterior stops. About 3 mm of clearance is recommended between the bumper and the teeth to allow proper lip contact with minimum discomfort.
There should be enough looseness in the molar tubes to allow the patient to insert the appliance easily and to promote active lip pressure and manipulation.
During treatment, the lip bumpers are activated so that one molar is rotated while the other is distalized.
The maxillary bite plane must be fitted to permit unhindered tooth eruption. Therefore, no wires or clasps should cross the occlusion and interfere with eruption where vertical development is desired. Occlusal acrylic may be added in certain areas to prevent eruption.
Selective extraction of primary teeth is an integral part of this treatment philosophy. “E-space” is conserved and maximized with sequential extraction. Since crowding most often occurs in the anterior regions, selective removal of primary teeth can encourage a distal eruptive pattern of the successive cuspids and premolars. Generally, no deciduous tooth should be extracted until one-half of the root of the succedaneous tooth has developed.
Bite Planes
The maxillary anterior bite plane impedes the eruption of the upper anterior teeth and permits eruption of the posterior teeth in low-angle cases.
Bite planes also supplement anterior or posterior anchorage when necessary.
Selective Extraction of Primary Teeth
Selective extraction encourages distobuccal eruption of the succedaneous cuspids and premolars, and uncrowds the anterior teeth by removing the restrictions of displaced permanent teeth and over-retained primary teeth.
Conclusion
Flexible lip bumpers are designed to be used in both arches. They are easily engaged and can effectively control molar rotation and distal movement. Therefore, they provide a viable alternative to the rigid bumper and the transpalatal arch, and they can be used as a source of anchorage or molar activation.
Arch development, relief of crowding, the “headgear effect,” and the “Frankel effect” can all be achieved with this therapy. Patient compliance is encouraged, while chairtime is reduced compared to other techniques. Treatment can be completed at an earlier age, with less need for extraction of permanent teeth or extensive fixed-appliance mechanotherapy.
Marcel Korn, DMD, is a diplomate of the American Board of Orthodontics, a member of the College of Diplomates of the American Board of Orthodontics, a member of the Angle Society of Orthodontists, and a fellow in the International College of Dentists. He maintains private practices in Boston and Fitchburg, Mass, and he is on the faculty at Tufts University School of Dental Medicine (Boston) in both the Department of Postgraduate Orthodontics and the Gelb Cranio-Mandibular Pain Center. He can be reached at [email protected].








