
by M. Constance B. Greeley, DDS
Improving treatment efficiency with OrthoCAD iQ technology
The idea of presetting brackets is not a new one for our practice. We first delved into indirect bonding a decade ago with some degree of success. However, as the practice grew, it became impractical to dedicate a technician to this procedure or to allocate doctor resources when it seemed better to utilize that time “at the chair.”
When the OrthoCAD iQ™ process became available we were skeptical, as it arrived on the heels of enormous change for us. We were switching from conventional bracket systems to the friction-free Damon system, and the learning curve was somewhat steep. During this kind of transition, new technology overlaps old technology and staff confusion can often ensue.
I had to be convinced, and I had to convince my partner as well. Two years ago we had again experimented with an in-house indirect bonding technique. My partner worked out every detail and trained the staff, but we weren’t impressed with the results or the efficiency. We weren’t in a hurry to subject the staff to yet again another challenging situation. They had to be convinced as well.
 |
| M. Constance B. Greeley, DDS |
An Idea That Works
Like so many things in our field, a good idea needs to be translated to a workable scenario or it will just remain a good idea. Cadent, maker of OrthoCAD iQ, made this idea work. So we brought our technical staff to see the OrthoCAD iQ operation at Cadent’s headquarters in Carlstadt, NJ. This is not a requirement, but something we opted to do. Then we allocated a day for training at our office, giving every technician a chance to utilize the tray system for new patients. We explained to the patients ahead of time that they were participating in a new technology, and we were pleased with the positive response.
The OrthoCAD system uses 3D software to create virtual models. While others can do that, this program allows the practitioner to essentially achieve bracket positions by adjusting tooth position and not by moving the bracket. In the process, brackets are adapted to varying tooth morphology using prescribed customized bondable bracket bases.
Clinical Application
What does this mean for you and your patients? It means that when you sit down to look at your setups, you can customize the bracket position for that particular patient
- without leaning over the patient;
- without interruptions; and
- without saliva, cheeks, and tongue issues.
It also allow you to
- look at your case from every angle;
- think about rotations, smile lines, bite opening, bite closing, and smile arcs; and
- select torques ahead of time, saving months of treatment time.
Now, as we progress through wires, tooth positions are more accurate relative to the intended occlusion. Repositioning and “tweaking” are minimized or eliminated. Treatment moves along a steady and efficient line, rather than in an interrupted pattern of forward and backward steps.
The patient reaction has been overwhelmingly positive. In our practice, we take the time to explain the process to patients during the consultation. It enhances the value of our treatment in the patient’s eyes and motivates them to cooperate.
Sample Cases
The following two cases illustrate a smooth course of treatment as a result of good torque planning, specific bracket placement, and good patient cooperation. Case 1 had no broken brackets in the first 9 months of treatment. Case 2 had one broken bracket in the first year of treatment. Both cases have had four archwire changes to date: .014 copper NiTi, .014 x .025 copper NiTi, .018 x .025 copper NiTi, and .019 x .025 steel. Case 1 had no bracket repositioning; case 2 had two brackets repositioned (Nos 4 and 11 were moved to a more mesial position).
Now, we typically don’t miss these rotations, because our computer-guided bracket-placement cases often require no bracket repositioning. Initially, appointments are 10 weeks apart. Once we insert steel wires, we usually see the patient every 4 to 6 weeks, especially if he or she is wearing elastics. The use of self-ligating Damon mechanics, coupled with the OrthoCAD technology, has made treatment more efficient and more predictable for both our staff and our patients.
We need to get over the idea that orthodontic treatment has to be arduous to be worthwhile. OrthoCAD iQ is a tool we can use to streamline treatment and provide patients with the experience they want and deserve in the new millennium.
M. Constance B. Greeley, DDS, is currently the treasurer of the Middle Atlantic Orthodontic Society and is past president of the Delaware State Dental Society. She is a diplomate of the American Board of Orthodontics. She has no financial interest in any of the products mentioned. She can be reached at
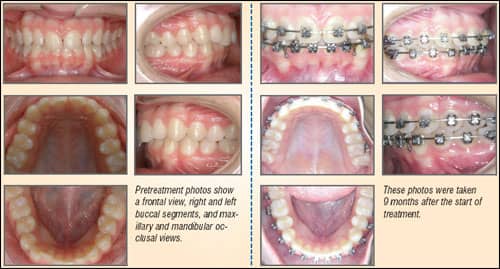 |
| Case 1: The female patient is 14 years and 2 months old. |
 |
| Case 2: This male patient is 31 years old. |








