
Good intra- and extra-oral images are critical to the diagnosis, treatment planning, and execution of orthodontic cases in a modern orthodontic setting. As models have gone digital, we need the photographs to verify the occlusion and facial balance at the start of treatment. In a busy orthodontic practice, it is common to view not only the chart but the photographs of the patient at each treatment visit in order to assess progress.
Over the years, the best intraoral images have been those where the source of light is near the lens, meaning a ring light or some variation thereof. The reason for this is that when the source of light is off center to the lens, shadows will be created that affect the image. For example, if you are trying to take a direct buccal picture of the right side occlusion with a cheek retractor in place, it is hard for the cheek not to get in the way of the flash situated to the left of the lens. The light will not be evenly distributed over the teeth and the distal part of the mouth could be darker.
Camera companies that specialize in dental photography have compensated for this situation well, but the physical and optical issues are inherent to the design of the cameras. The problem with today’s ring light system cameras is that they are utilized with traditional SLR cameras and lenses, which can make them big, heavy, and somewhat cumbersome.
So what would be the ideal camera for intraoral use? In theory, the best combination would be a lightweight camera that is small and incorporates a ring light! Along comes Canon with a new system that has just that.
Called “mirrorless,” this new breed of camera doesn’t have an optical viewfinder, meaning it doesn’t need mirrors or prisms that reflect light from the lens to the eye. As a result, the cameras are smaller than a traditional SLR and lightweight.
Wanting to see if this new camera type could be adopted for use in dental photography, I took it for a test run. My practice tested the Canon M10 mirrorless camera with the EF-M 28 mm Macro lens with built-in ring light (camera loaned courtesy of CEO Barry Litwin of Adorama Camera, New York). The goal was to see if good intraoral images could be obtained with the camera and lens straight out-of-the-box, with minimal setting requirements.
A Review
Is the camera small and lightweight? Of their mirrorless cameras, the M10 is the simplest and lightest weight camera available in this category. According to Canon, it weighs approximately 10.6 ounces. With the 4.6-ounce lens attached, the camera still weighs less than a pound. In comparison, Canon’s smallest and lightest SLR camera weighs 14.4 ounces, and that is just the body alone without lens or ring light. With the lens, we’re looking at handling a weight closer to 2 pounds or more. Even if 2 pounds is not excessively heavy, maneuvering a lighter-weight camera is easier.

Figure 1: Take camera off automatic setting.
What tweaks need to be made to the settings for orthodontic use? The nice feature of this camera is that it is simple, and minimal settings are required. That being said, while using it in our office, we discovered four simple tweaks to the default settings that can help produce good orthodontic images that meet our diagnostic needs.

Figure 2: Set to Av, or aperture priority.
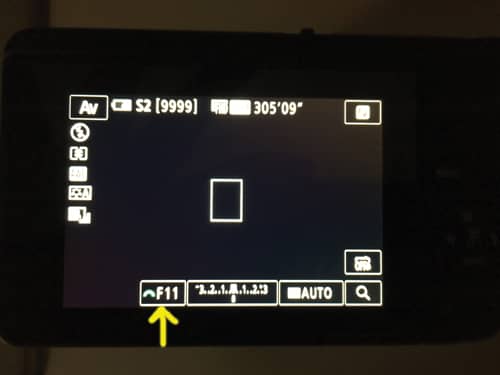
Figure 3: In Av mode, the f-stop can be adjusted.
First, take the camera off the automatic setting and change to “Creative Assist Mode” (Figure 1). Second, while in this mode, the camera has to be set to Av, or aperture priority (Figure 2). As a result, you can set the f-stop of the camera (Figure 3), and the camera sets the shutter speed accordingly. The reason for this is that you want good depth of focus—depth of field in photo lingo. The higher the number, the higher the depth of field and the more of the image will be in focus. If you left the camera to its own volition, on automatic, it sets too low an f-stop. You have to force it to set an adequate depth of field. The problem is that if the number is too high, the camera sets too low of a shutter speed to compensate for the lack of light, and the images are blurry. (It is hard to hand-hold a camera, and keep it as steady as it needs to be kept, with a shutter speed set at 1/15 of a second. The resulting images are unlikely to be clear.) We found that the camera, when set at f11, set a speed of 1/60 of a second, which will work effectively. The fourth and last tweak to the settings we advise after testing this model is to choose the smallest possible image size, without going under 1 MB (Figure 2). Orthodontic images do not have to be large. An image that is 1 MB is perfectly adequate for our needs. Besides, if you are using the cloud, you want image files to be small to reduce upload and download time. In this case, S2 was the smallest size, roughly 4 MB. We left the remaining settings at factory default.

Figure 4: Camera shown without ring light activated.

Figure 5: Camera shown with ring light at maximum brightness.
Is the light bright enough for intraoral use? With the settings adjusted, we can focus on the effectiveness of the light. And here we run into a potential issue. Figures 4 and 5 show the camera with and without the ring light at maximum brightness. Meanwhile, Figure 6 shows how far the flash is from the lens when extended, and the shadows created are unacceptable; thus the flash cannot be used. This means we are limited to relying solely on the ring light for all the light necessary to illuminate the mouth. Although the ring light casts enough light to illuminate the intraoral environment, the light is not as intense as that coming from a flash; the camera in turn compensates for this. The resultant images are definitely grainy, but this is of no consequence to our needs. So the bottom line with respect to light? The system can illuminate the intraoral environment adequately and with flat, shadowless light (Figure 7).

Figure 6: Shown here, the distance between the flash and lens when extended.
Does the camera take good extraoral images? Figure 7 shows frontal rest, profile, and frontal smile images. These were taken without the flash, again using only the ring light to illuminate the subject. The pictures, although grainy, are perfectly adequate for our orthodontic needs and there are no shadows, especially in the profile image, to affect facial balance assessment.
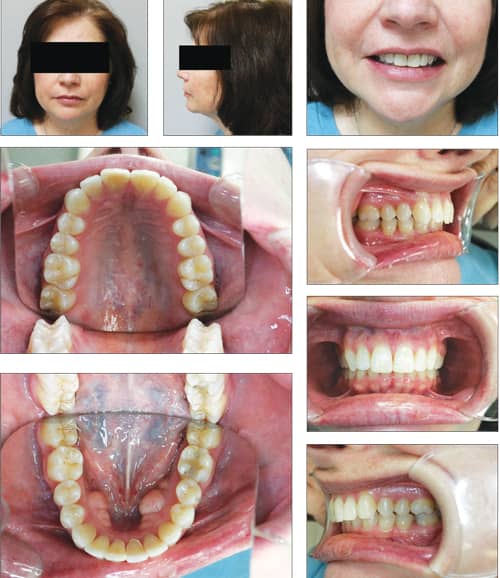
Figure 7: Images taken with the Canon M10 mirrorless camera with the EF-M 28 mm Macro lens with built-in ring light.
Does the camera system allow you to zoom in and out to focus? The lens is a fixed focus 28 mm lens which does not have zoom capability. This is a weakness of the system because in order for you to crop the image to the teeth, without mirror edges, retractors, etc, you have to be very close to the patient, which can be disconcerting. The system was designed for macro photography, not specifically for intraoral use. A longer lens (50+ mm) would be better because it would mean that you would not have to be so close to the patient when framing the images.
Conclusion
An off-the-shelf camera like the Canon M10 camera and 28 mm lens with ring light is a viable system for orthodontic photography, but not perfect. The pros are that the camera is small and lightweight; the ring light projects flat, shadowless light; and the camera can be used straight out-of-the-box with minimal setting changes. The cons are that you cannot use the flash because of shadow creation, the images are grainy, and there is no zoom function to allow you to take images further from the patient. In addition, you will have to set and calibrate the system on your own, as opposed to a turnkey solution offered by dental photography suppliers.
I talked to Matt Glassgold, of dental photography supplier Lester Dine Corp, to get his take on the images we took with this system. While he agreed that the Canon M10 combined with a lens attachment and built-in ring flash is an interesting option, and appears to have some intraoral photography capabilities, it falls short in his opinion.
“Its price point is close to the less expensive digital SLR options, but those cameras also have a true macro lens and ring flash. However, the SLR cameras are superior in terms of lighting, depth of field, and range of photography. The digital SLRs are able to more closely frame anterior, lateral, buccal, and occlusal photography while also photographing the intraoral quadrant subject,” Glassgold says, adding that he doesn’t believe the M10-based system is simplified enough to compete with modified handheld digital cameras which can be photographically superior in terms of range of photography and lower price.
“Based on its price point and photographic ability,” Glassgold says, “it’s my belief that the M10/built-in ring flash concept is a work in progress rather than a truly viable solution for a busy [dental professional].”
Based on my experience, the pros and cons listed above, and the comments of Glassgold, I rate this camera system at 7.5/8 out of 10 for orthodontic use. It would be nice if camera manufacturers recognized that the niche markets, like the medical and dental markets, could benefit from a simple, light, inexpensive ring light camera system. While Shofu Dental Corp, San Marcos, Calif, has a camera that meets the technical requirements of such a system, it is prohibitively expensive. Decades ago, the Japanese company Yashica (later Kyocera) offered the Dental Eye, which met both the technical requirements and cost parameters of most practices, but it is no longer available new. I can only hope that a company resurrects that product in a digital version.
In the meantime, the lesson here is to keep an eye on off-the-shelf options made for the general consumer in this and other product categories. As innovation in digital technologies continues, there are systems that may meet, or can be adapted to meet, our needs while being cost-effective. OP
 Howard A. Fine, DMD, MMSc, has served on the editorial advisory board of Orthodontic Products since its inception. He has private practices in both Mount Kisco and Katonah, NY, where he has practiced for 29 years. He served as assistant clinical professor of orthodontics at the Department of Orthodontics, Montefiore Medical Center, Bronx, NY. His areas of interest include digital imaging and computer technology. Fine has written numerous articles on these topics for this magazine.
Howard A. Fine, DMD, MMSc, has served on the editorial advisory board of Orthodontic Products since its inception. He has private practices in both Mount Kisco and Katonah, NY, where he has practiced for 29 years. He served as assistant clinical professor of orthodontics at the Department of Orthodontics, Montefiore Medical Center, Bronx, NY. His areas of interest include digital imaging and computer technology. Fine has written numerous articles on these topics for this magazine.








