
by Stephen Tracey, DDS, MS
An alternative to orthognathic surgery

After struggling for years to maintain anchorage during orthodontic treatment, orthodontists have now come to appreciate the benefits of miniscrew anchorage. Miniscrews are small, easily placed, well-tolerated by patients, and easily removed. More importantly, they provide absolute anchorage and can be immediately loaded. Clinical situations frequently enhanced by miniscrew anchorage include closure of space from extracted or missing teeth, intrusion and extrusion of single and multiple teeth, buccal crossbite correction, and molar uprighting. Benefits of incorporating miniscrew anchorage into orthodontic treatment include reduced cooperation requirements, fewer appointments, decreased treatment times, and superior overall results.
In some cases, miniscrew anchorage enables orthodontists to treat patients who would have previously required orthognathic surgery with more conservative, nonsurgical treatment plans. Examples of such treatment include closure of anterior open bites, reduction of gummy smiles that are the result of vertical maxillary excess, and full arch retraction in selected Class III cases.
While surgical assistance with these types of cases is often considered essential, many patients are hesitant to undergo orthodontic treatment that incorporates orthognathic surgery. Possible complications of surgery include excessive bleeding, swelling, nausea, vomiting, weight loss, and infection. Additionally, nerve damage may result in temporary—or even permanent—numbness of the face. Furthermore, surgeries involving the upper jaw have the potential to adversely change the shape of the nose. Also, from an economic standpoint, the additional fees associated with surgery put treatment out of reach for many patients, particularly those without medical insurance. Downtime is also an issue in most instances, as some patients are unable to take the needed 2 weeks off from work to recover. Needless to say, if offered a choice between surgical and nonsurgical treatment plans, most patients prefer to avoid surgery if at all possible.
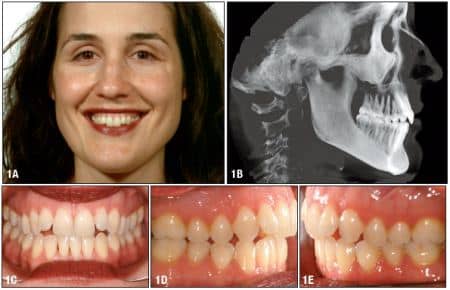
Figure 1: This adult female presented with a Class II malocclusion, mild upper and lower crowding, a narrow upper arch, and a mildly steep mandibular plane angle. Her chief complaint was a gummy smile combined with an anterior open bite.

Figure 2: Miniscrews were placed buccally between the upper second bicuspids and first molars, slightly above the mucogingival junction. Intrusive force was provided by attaching 5-mm, 150-gm double-delta NiTi coils.

Figure 3: 16 weeks later, miniscrews were placed on the lingual surface of the alveolar process. Figure 4: After another 16 weeks, the open bite was closed. Figure 5: The patient wore vertical elastics to seat the occlusion.

Figure 6: The patient was debanded at 18 months with an aesthetically pleasing and fully functional occlusion.

Figure 7: An adult female presented with a significant Class III malocclusion, a prognathic mandible, upper spacing, and lower crowding. I noted black triangles in the lower anterior teeth due to a combination of triangular-shaped lower incisors and gingival recession.

Figure 8: 5-mm, 250-gm single-delta with swivel NiTi coils were attached from the miniscrew heads to the miniscrew’s crimpable posts crimped onto the lower archwire. Figure 9: The patient was debanded and equilibrated at 17 months.
In this article, I will examine two potential surgery cases that I treated nonsurgically with the assistance of miniscrew anchorage.
Case 1: Gummy Smile and Anterior Open Bite
An adult female presented with a Class II malocclusion, mild upper and lower crowding, a narrow upper arch, and a mildly steep mandibular plane angle (Figures 1A to 1E). Her chief complaint was a gummy smile combined with an anterior open bite. I noted the difficulty of closing the anterior open bite, while at the same time reducing excess gingival display, and offered the patient a choice between two orthodontic treatment plans. One treatment plan incorporated a maxillary impaction surgery, and the other would not involve surgery, but instead use miniscrew anchorage. After much discussion of the pros and cons of each treatment plan, the patient elected to proceed with the nonsurgical approach.
It should be noted that attempting to treat this case nonsurgically with miniscrew-assisted orthodontics proved to be a challenge at best. Normal protocols to close an anterior open bite involve posterior intrusion combined with some extrusion of the anterior teeth. However, in this case the patient also exhibited excess gingival display as result of anterior vertical maxillary excess, necessitating the need for anterior intrusion. If not ideally managed, any anterior intrusion could potentially exacerbate the open bite.
Treatment
I initiated full orthodontic treatment, using a combination of Ormco Ice and Ormco’s Damon Q bracket system to meet the aesthetic needs of the patient. The appliance slot size was .022 x .028 to take advantage of the considerably greater control afforded by .019 x .025 TMA archwires during the intrusion phase of treatment. I leveled and aligned the upper arch with progressive archwires up to a .019 x .025 TMA.
Miniscrew Placement
I decided to start the miniscrew treatment with posterior intrusion to close the anterior open bite before addressing the gummy smile. Consequently, I placed VectorTAS 8-mm miniscrews buccally between the upper second bicuspids and first molars, slightly above the mucogingival junction. Intrusive force was provided by attaching VectorTAS 5-mm, 150-gm double-delta NiTi coils from the miniscrews, looping them down and around the main archwire and back to the screw heads (Figures 2A and 2B, page 18). Due to the buccal placement of the initial miniscrews, I anticipated that in addition to the expected intrusion, some posterior expansion would also occur.
At an appointment 16 weeks later, I observed significant posterior intrusion along with some expansion and buccal flaring. To increase the amount of intrusive force, as well as lift the lingual cusps of the upper posterior teeth, I placed VectorTAS 8-mm miniscrews on the lingual surface of the alveolar process between the first and second molars. I bonded buttons to the lingual surfaces of the molars, and stretched VectorTAS 5-mm, 150-gm double-delta NiTi coils from the buttons into the undercuts between the two delta-shaped heads on the miniscrews (Figure 3).
Two appointments and another 16 weeks later, the anterior open bite was closed as the result of posterior intrusion and autorotation of the mandible. I initiated anterior intrusion by placing VectorTAS 8-mm miniscrews buccally between the upper lateral incisors and cuspids slightly above the mucogingival junction (Figure 4). Although it is preferable to apply intrusive forces with NiTi coils due to the predictably light and continuous forces they produce, in this case I used elastomeric chain to meet the patient’s aesthetic demands. Once the upper arch was positioned satisfactorily and the excessive gingival display reduced, I removed the intrusive forces and replaced them with .012 ligature wires to maintain the maxillary intrusion. The patient wore vertical elastics to seat the occlusion (Figure 5).
The patient was debanded at 18 months with an aesthetically pleasing and fully functional occlusion (Figures 6A to 6D).
Case 2: Class III Malocclusion
An adult female presented with a significant Class III malocclusion, a prognathic mandible, upper spacing, and lower crowding. I noted black triangles in the lower anterior teeth due to a combination of triangular-shaped lower incisors and gingival recession (Figures 7A to 7E). I discussed surgical and nonsurgical treatment options with the patient, who elected to forgo surgery in lieu of miniscrew-assisted orthodontics. I determined that, by combining interproximal reduction in the lower arch (which also helped reduce the black triangles) with en masse retraction of the lower dentition, it would be possible to achieve a satisfactory result without surgery.
Treatment
I initiated full orthodontic treatment, using a combination of Ormco Ice and Orthos Titanium brackets to meet the aesthetic needs of the patient. Appliance slot size was .022 x .028 to take advantage of the control afforded by .019 x .025 TMA archwires during en masse retraction of the lower arch. I leveled and aligned the upper and lower arches with progressive archwires up to .019 x .025 TMA.
Miniscrew Placement
I accomplished en masse retraction of the lower arch along with space closure that resulted from interproximal reduction of the lower incisors with the assistance of VectorTAS 10-mm miniscrews placed vertically in the oblique ridges just lateral to the mandibular second molars utilizing a contra-angle driver. I attached VectorTAS 5-mm, 250-gm single-delta with swivel NiTi coils from the miniscrew heads to the miniscrew’s crimpable posts crimped onto the lower archwire (Figures 8A and 8B). Initial placement of the posts was between the first and second bicuspids, but subsequently they were repositioned between the cuspids and first bicuspids as the activation of the NiTi coils diminished with retraction of the lower dentition toward the miniscrews. I performed miniscrew-assisted retraction of the lower arch over a period of 7 months.
For a complete list of companies that sell miniscrews, visit our online Buyer’s Guide.
After the miniscrews were removed, I used vertical elastics to seat the posterior occlusion. The patient was debanded and equilibrated at 17 months with a healthy, visually appealing, and fully functional occlusion (Figures 9A to 9E).
In summary, refinements in technique, along with development of advanced miniscrew systems designed specifically for orthodontic anchorage, have brought universal acceptance of skeletal anchorage. Today’s miniscrew treatment solutions are helping clinicians address complex orthodontic cases more easily and quickly than ever before, while delivering precision outcomes. More importantly, miniscrew-assisted orthodontics has brought new hope to patients wishing to avoid costly and potentially painful surgery.
Stephen Tracey, DDS, MS, a VectorTAS provider, is in private practice in Upland, Calif. He is a visiting professor of orthodontics at the University of Ferrara in Ferrara, Italy. He was one of the first orthodontists in North America to incorporate miniscrew anchorage into orthodontics. He can be reached at







